

Clinicopathologic features of remnant gastric cancer after curative distal gastrectomy according to previous reconstruction method: a retrospective cohort study
- PMID: 31785616
- PMCID: PMC6885312
- DOI: 10.1186/s12957-019-1740-3
Clinicopathologic features of remnant gastric cancer after curative distal gastrectomy according to previous reconstruction method: a retrospective cohort study
Abstract
Background: Survival rate of patients treated for gastric cancer has increased due to early detection and improvements of surgical technique and chemotherapy. Increase in survival rate has led to an increase in the risk for remnant gastric cancer (RGC). The purpose of this study was to investigate clinicopathologic features of RGC according to previous reconstruction method and factors affecting the interval from previous curative distal gastrectomy for gastric cancer to RGC occurrence.
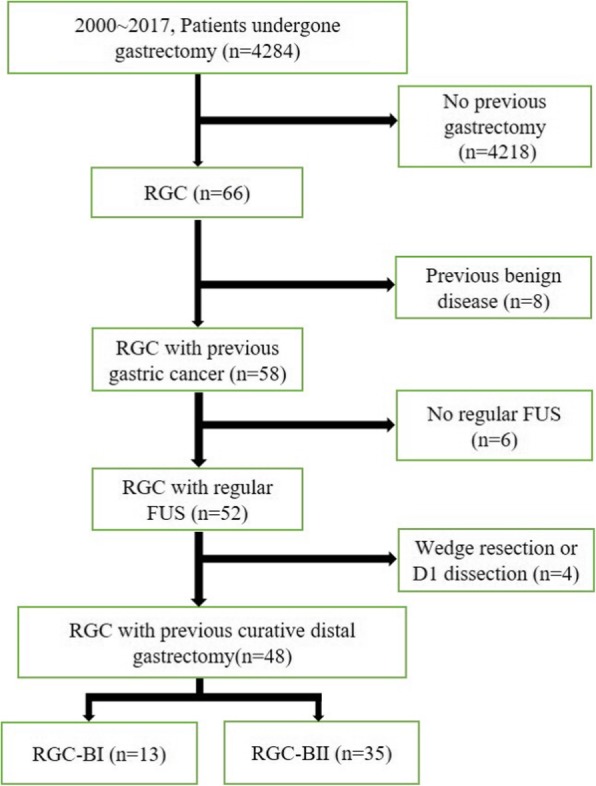
Methods: Medical records of patients diagnosed with RGC at Yeungnam University Medical Center from January 2000 to December 2017 who had a history of distal gastrectomy with D2 LN dissection due to gastric cancer were reviewed retrospectively.
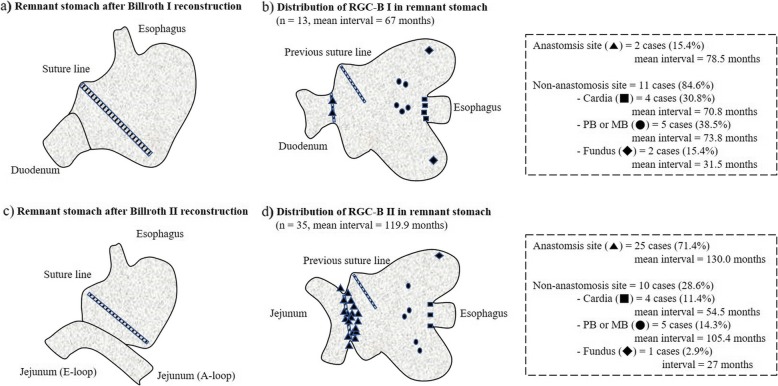
Results: Forty-eight patients were enrolled in this study. The mean interval of 48 RGC patients was 105.6 months (8.8 years). RGC after Billroth II reconstruction recurred more often at anastomosis site than RGC after Billroth I reconstruction (p = 0.001). The mean interval of RGC after Billroth I reconstruction was 67 months, shorter than 119 months of RGC after Billroth II reconstruction (p = 0.003). On the contrary, interval showed no difference according to stage of previous gastric cancer, remnant gastric cancer, or sex (p = 0.810, 0.145, and 0.372, respectively).
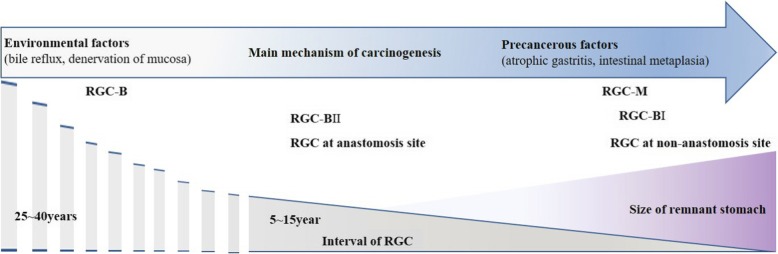
Conclusions: RGC after Billroth I reconstruction tends to arise earlier at non-anastomosis site than RGC after Billroth II. Therefore, we should examine non-anastomosis site carefully from the beginning of surveillance after gastric cancer surgery with Billroth I reconstruction for better outcome.
Keywords: Reconstruction; Recurrence interval; Remnant gastric cancer.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Progression of remnant gastric cancer is associated with duration of follow-up following distal gastrectomy.World J Gastroenterol. 2012 Jun 14;18(22):2832-6. doi: 10.3748/wjg.v18.i22.2832. World J Gastroenterol. 2012. PMID: 22719193 Free PMC article.
-
Functional outcomes according to the size of the gastric remnant and type of reconstruction following laparoscopic distal gastrectomy for gastric cancer.Gastric Cancer. 2011 Aug;14(3):279-84. doi: 10.1007/s10120-011-0046-0. Epub 2011 Apr 26. Gastric Cancer. 2011. PMID: 21519869
-
Surgical Resection of Remnant Gastric Cancer Following Distal Gastrectomy: A Retrospective Clinicopathological Study.Ann Surg Oncol. 2016 Feb;23(2):511-21. doi: 10.1245/s10434-015-4678-x. Epub 2015 Jun 24. Ann Surg Oncol. 2016. PMID: 26104543
-
Current status in remnant gastric cancer after distal gastrectomy.World J Gastroenterol. 2016 Feb 28;22(8):2424-33. doi: 10.3748/wjg.v22.i8.2424. World J Gastroenterol. 2016. PMID: 26937131 Free PMC article. Review.
-
Laparoscopic gastrectomy for remnant gastric cancer: a comprehensive review and case series.Gastric Cancer. 2016 Jan;19(1):287-92. doi: 10.1007/s10120-014-0451-2. Epub 2014 Dec 13. Gastric Cancer. 2016. PMID: 25503677 Review.
Cited by
-
Success Rate and Factors Associated With Surveillance Endoscopy After Proximal Gastrectomy With Double-Tract Reconstruction: A Retrospective Multicenter Cohort Study.J Gastric Cancer. 2025 Jul;25(3):466-477. doi: 10.5230/jgc.2025.25.e32. J Gastric Cancer. 2025. PMID: 40631475 Free PMC article.
-
Gastric Remnant Carcinosarcoma: Case Report and Review of the Literature.J Gastrointest Cancer. 2021 Mar;52(1):336-341. doi: 10.1007/s12029-020-00447-3. J Gastrointest Cancer. 2021. PMID: 32607961 Review. No abstract available.
-
Leptomeningeal disease in glioblastoma: endgame or opportunity?J Neurooncol. 2021 Nov;155(2):107-115. doi: 10.1007/s11060-021-03864-x. Epub 2021 Oct 8. J Neurooncol. 2021. PMID: 34623599
-
T stage and venous invasion are crucial prognostic factors for long-term survival of patients with remnant gastric cancer: a cohort study.World J Surg Oncol. 2021 Sep 27;19(1):291. doi: 10.1186/s12957-021-02400-5. World J Surg Oncol. 2021. PMID: 34579733 Free PMC article.
-
3D laparoscopic-assisted vs open gastrectomy for carcinoma in the remnant stomach: A retrospective cohort study.World J Gastrointest Surg. 2022 Aug 27;14(8):754-764. doi: 10.4240/wjgs.v14.i8.754. World J Gastrointest Surg. 2022. PMID: 36157370 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
