

Global Trends in Anaphylaxis Epidemiology and Clinical Implications
- PMID: 31786255
- PMCID: PMC7152797
- DOI: 10.1016/j.jaip.2019.11.027
Global Trends in Anaphylaxis Epidemiology and Clinical Implications
Abstract
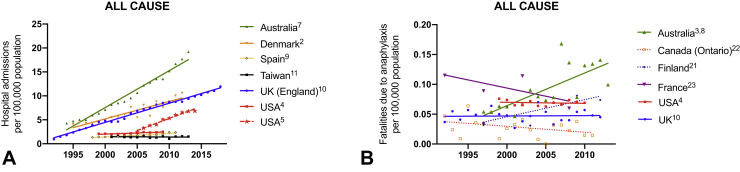
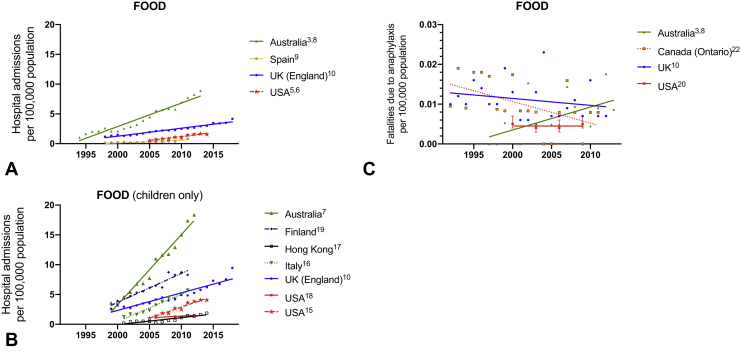
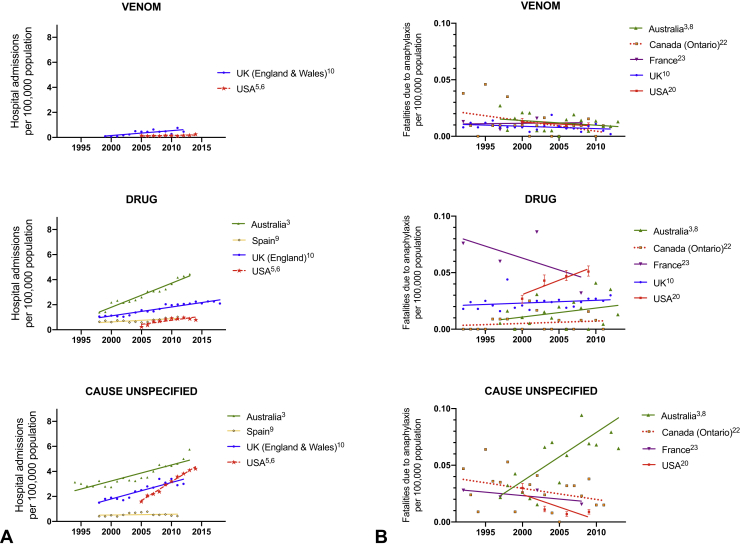
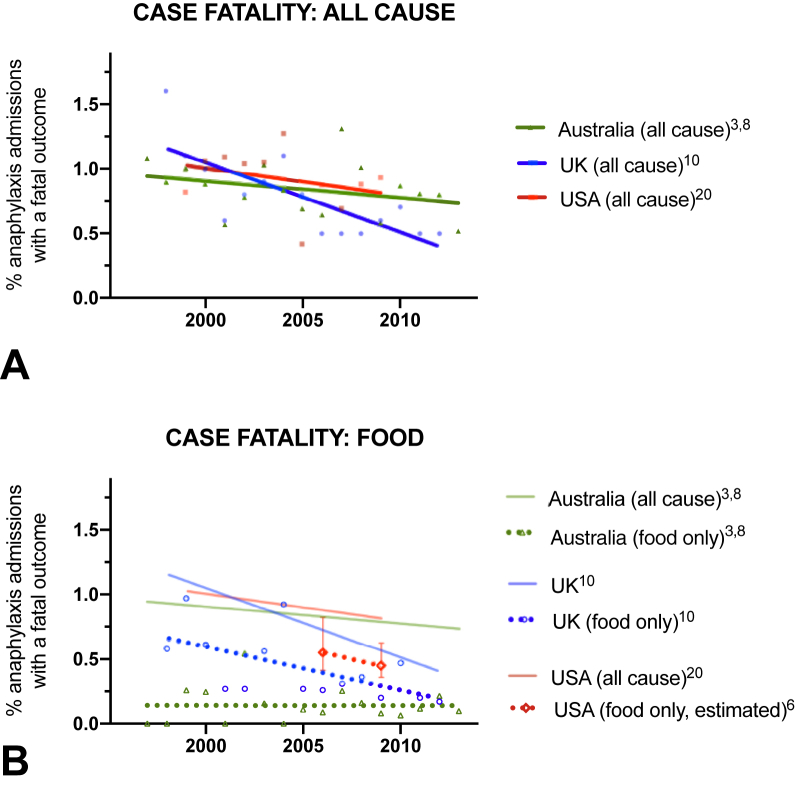
The true global scale of anaphylaxis remains elusive, because many episodes occur in the community without presentation to health care facilities, and most regions have not yet developed reliable systems with which to monitor severe allergic events. The most robust data sets currently available are based largely on hospital admissions, which are limited by inherent issues of misdiagnosis, misclassification, and generalizability. Despite this, there is convincing evidence of a global increase in rates of all-cause anaphylaxis, driven largely by medication- and food-related anaphylaxis. There is no evidence of parallel increases in global all-cause anaphylaxis mortality, with surprisingly similar estimates for case-fatality rates at approximately 0.5% to 1% of fatal outcomes for hospitalizations due to anaphylaxis across several regions. Studying regional patterns of anaphylaxis to certain triggers have provided valuable insights into susceptibility and sensitizing events: for example, the link between the mAb cetuximab and allergy to mammalian meat. Likewise, data from published fatality registers can identify potentially modifiable risk factors that can be used to inform clinical practice, such as prevention of delayed epinephrine administration, correct posturing during anaphylaxis, special attention to populations at risk (such as the elderly on multiple medications), and use of venom immunotherapy in individuals at risk of insect-related anaphylaxis.
Keywords: Anaphylaxis; Biphasic; Epidemiology; Food allergy; Time trends.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Asai Y., Yanishevsky Y., Clarke A., La Vieille S., Delaney J.S., Alizadehfar R. Rate, triggers, severity and management of anaphylaxis in adults treated in a Canadian emergency department. Int Arch Allergy Immunol. 2014;164:246–252. - PubMed
-
- Motosue M.S., Bellolio M.F., Van Houten H.K., Shah N.D., Campbell R.L. Increasing emergency department visits for anaphylaxis, 2005-2014. J Allergy Clin Immunol Pract. 2017;5:171–175.e3. - PubMed
-
- Motosue M.S., Bellolio M.F., Van Houten H.K., Shah N.D., Li J.T., Campbell R.L. Outcomes of emergency department anaphylaxis visits from 2005 to 2014. J Allergy Clin Immunol Pract. 2018;6:1002–1009.e2. - PubMed
-
- Jeppesen A.N., Christiansen C.F., Froslev T., Sorensen H.T. Hospitalization rates and prognosis of patients with anaphylactic shock in Denmark from 1995 through 2012. J Allergy Clin Immunol. 2016;137:1143–1147. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
