

High-risk Meningioma: Initial Outcomes From NRG Oncology/RTOG 0539
- PMID: 31786276
- PMCID: PMC7117785
- DOI: 10.1016/j.ijrobp.2019.11.028
High-risk Meningioma: Initial Outcomes From NRG Oncology/RTOG 0539
Abstract
Background: Phase 2 cooperative group meningioma trial assessing the safety and efficacy of risk-adaptive management strategies. This is the initial analysis of the high-risk cohort.
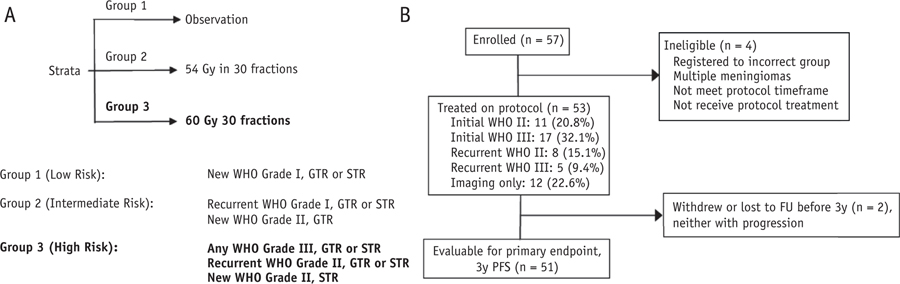
Methods and materials: High-risk patients were those with a new or recurrent World Health Organization (WHO) grade III meningioma of any resection extent, recurrent WHO grade II of any resection extent, or new WHO grade II after subtotal resection. Patients received intensity-modulated radiotherapy (IMRT) using a simultaneous integrated boost technique (60 Gy high dose and 54 Gy low dose in 30 fractions). Three-year progression-free survival (PFS) was the primary endpoint. Adverse events (AEs) were scored per NCI Common Terminology Criteria for Adverse Events version 3.
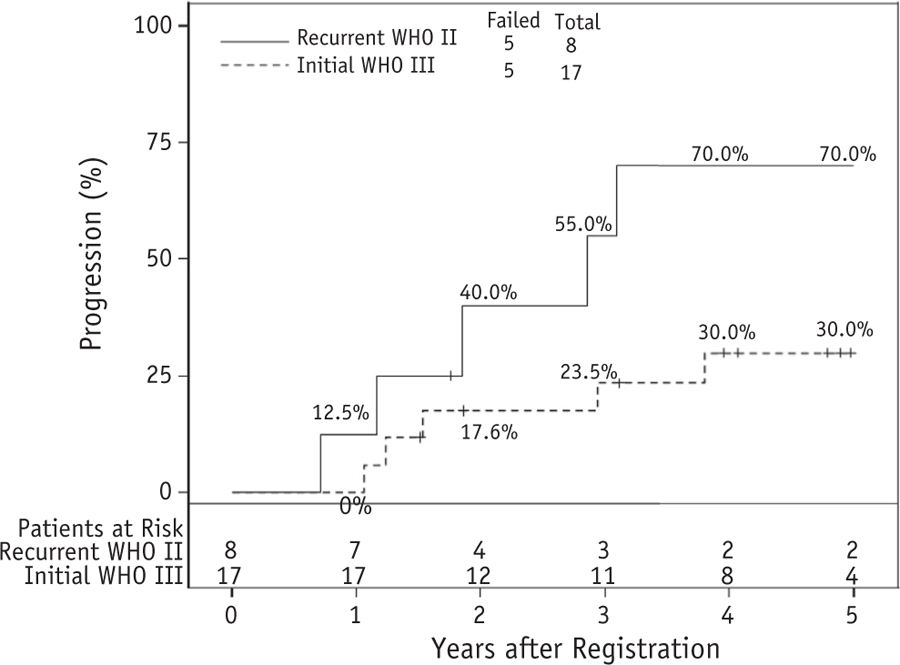
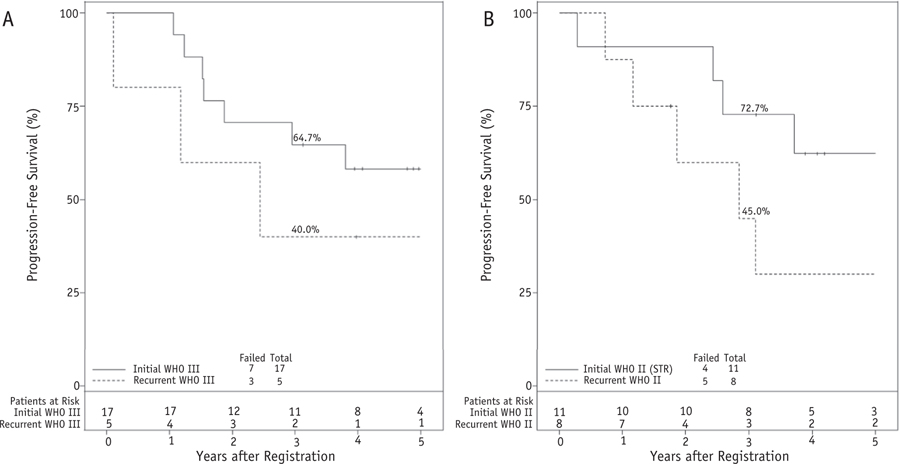
Results: Of 57 enrolled patients, 53 received protocol treatment. Median follow-up was 4.0 years (4.8 years for living patients). Two patients withdrew without progression before year 3; for the remaining 51 patients, 3-year PFS was 58.8%. Among all 53 protocol-treated patients, 3-year PFS was 59.2%. Three-year local control was 68.9%, and overall survival was 78.6%. Of 51 patients, 1 patient (1.9%) experienced a late grade-5 necrosis-related AE. All other acute (23 of 53 patients) and late (21 of 51 patients) AEs were grades 1 to 3.
Conclusions: Patients with high-risk meningioma treated with IMRT (60 Gy/30) experienced 3-year PFS of 58.8%. Combined acute and late AEs were limited to grades 1 to 3, except for a single necrosis-related grade 5 event. These results support postoperative IMRT for high-risk meningioma and invite ongoing investigations to improve outcomes further.
Trial registration: ClinicalTrials.gov NCT00895622.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures


References
-
- Claus EB, Bondy ML, Schildkraut JM, et al. Epidemiology of intracranial meningioma. Neurosurgery 2005;57:1088–1095; [discussion: 1088–1095]. - PubMed
-
- Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 2016;131:803–820. - PubMed
-
- Perry A, Stafford SL, Scheithauer BW, et al. Meningioma grading: an analysis of histologic parameters. Am J Surg Pathol 1997;21:1455–1465. - PubMed
-
- Perry A, Scheithauer BW, Stafford SL, et al. “Malignancy” in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer 1999;85:2046–2056. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
