

[Predictive factors of bacteraemia in the patients seen in emergency departments due to infections]
- PMID: 31786907
- PMCID: PMC6987628
- DOI: 10.37201/req/075.2019
[Predictive factors of bacteraemia in the patients seen in emergency departments due to infections]
Abstract
Objective: The aim of the study was to analyze predictive factors of bacteraemia in patients seen in the emergency department (ED) for an episode of infectious disease.
Methods: Observational, retrospective and descriptive analytical study of all blood cultures extracted in an ED in adult patients (≥ 18 years) seen in ED due to infec-tious disease from 1-1-2019 to 1-7-2019. The follow-up was carried out during 30 days. Thirty-eight variables for predicting bacteraemia were assessed. They covered epidemiological, comorbidity, functional, clinical and analytical factors. Univariate and multivariate logistic regression analysis was performed.
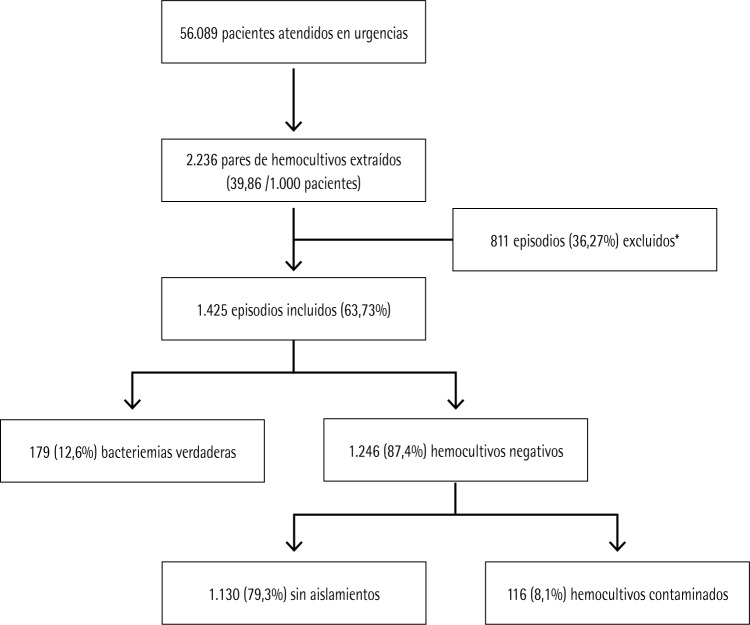
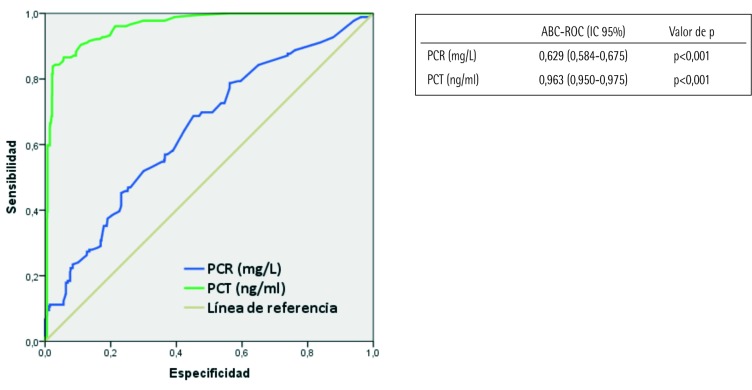
Results: A total of 1,425 blood cultures were finally enrolled in the study. Of those were considered true bacteremia 179 (12.6 %) and as negative blood cultures 1,246 (87.4 %). Amongst negatives, 1,130 (79.3%) without growth and 116 (8.1%) as contaminants blood cultures. Five variables were significantly associated with true bacteraemia: serum procalcitonin (PCT) ≥ 0.51 ng/ml [odds ratio (OR): 4.52; 95% confidence interval (CI): 4.20-4.84, P <.001], temperature > 38.3°C [OR:1.60; 95% CI:1.29-1.90, P <.001], systolic blood pressure (SBP) < 100 mmHg [OR:3.68; 95% CI:2.78-4.58, P <.001], septic shock [OR:2.96; 95% CI:1.78-4.13, P <.001] and malignancy [OR:1.73; 95% CI:1.27-2.20, P <.001].
Conclusions: Several factors evaluated in an initial assessment in the ED, including serum PCT, temperature, hypotension (with/without septic shock) and being malignancy, were found to predict true bacteraemia.
Objetivos: Analizar los factores predictivos de bacteriemia en los pacientes atendidos en el servicio de urgencias (SU) por un episodio de infección.
Pacientes y métodos: Estudio observacional, retrospectivo, descriptivo y analítico de todos los hemocultivos extraídos en un SU en los pacientes adultos (≥ 18 años) atendidos por infección desde el 1-1-2018 hasta el 1-7-2018. Se realizó seguimiento durante 30 días. Se analizaron 38 variables independientes (epidemiológicas, de comorbilidad, funcionales, clínicas y analíticas) que pudieran predecir la existencia de bacteriemia. Se realizó un estudio univariado y multivariante mediante regresión logística.
Resultados: Se incluyeron 1.425 episodios de hemocultivos extraídos. De ellos se consideraron como bacteriemias verdaderas 179 (12,6 %) y como HC negativos 1.246 (87,4 %). Entre los negativos, 1.130 (79,3%) no tuvieron crecimiento y 116 (8,1%) se consideraron contaminados. Cinco variables se asociaron de forma significativa como predictoras de bacteriemia verdadera: procalcitonina (PCT) sérica ≥ 0,51 ng/ml [odds ratio (OR): 4,52; intervalo de confianza (IC) al 95%: 4,20-4,84; p <0,001], temperatura > 38,3°C [OR: 1,60; IC al 95%: 1,29-1,90; p <0,001], presión arterial sistólica (PAS) < 100 mmHg [OR: 3,68; IC al 95%: 2,78-4,58; p <0,001], shock séptico [OR: 2,96; IC al 95%: 1,78-4,13; p <0,001] y la existencia de neoplasia [OR: 1,73; IC al 95%: 1,27-2,20; p <0,001].
Conclusiones: . Existen varios factores disponibles tras una primera valoración en el SU, entre ellos la PCT sérica, la temperatura, la hipotensión con/sin criterios de shock séptico y la existencia de neoplasia, que predicen la existencia de bacteriemia verdadera.
Keywords: Bacteraemia; Biomarkers; Blood cultures; C-reactive protein; Emergency Department; Predictive factors; Procalcitonin.
©The Author 2020. Published by Sociedad Española de Quimioterapia. This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)(https://creativecommons.org/licenses/by-nc/4.0/).
Conflict of interest statement
AJJ ha participado en reuniones científicas organizadas por Bayer, Boehringer, Esteve, GSK, Lilly, MSD, Pfizer, Tedec Meiji, Roche, Thermo Scientific Biomarkers, B.R.A.H.M.S. AG y Biomerieux.
Los autores declaran la ausencia de conflictos de intereses en relación con el presente artículo.
Figures
References
-
- Julián-Jiménez A, Supino M, López Tapia JD, Ulloa González C, Var-gas Téllez LE, González del Castillo J, et al. Puntos clave y contro-versias sobre la sepsis en los servicios de urgencias: propuestas de mejora para Latinoamérica. Emergencias 2019; 31:123-135. PMid: - PubMed
-
- Cisneros-Herreros JM, Cobo-Reinoso J, Puyol-Rojo M, Rodríguez-Baño J, Salavert-Lleti M. Guía para el diagnóstico y tratamiento del paciente con bacteriemia. Guías de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica (SEIMC). En-ferm Infecc Microbiol Clin. 2007; 25:111-30. DOI: 10.1016/S0213-005X(07)74242-8 - DOI - PubMed
-
- Ortega Romero M. Uso de antimicrobianos en urgencias: ¿hay margen de mejora? Emergencias 2018; 30:292-4. PMid: - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
