

Longitudinal Changes in Functional Connectivity of the Caudate Is Associated With Recovery From Bell's Palsy
- PMID: 31787890
- PMCID: PMC6853889
- DOI: 10.3389/fnagi.2019.00295
Longitudinal Changes in Functional Connectivity of the Caudate Is Associated With Recovery From Bell's Palsy
Abstract
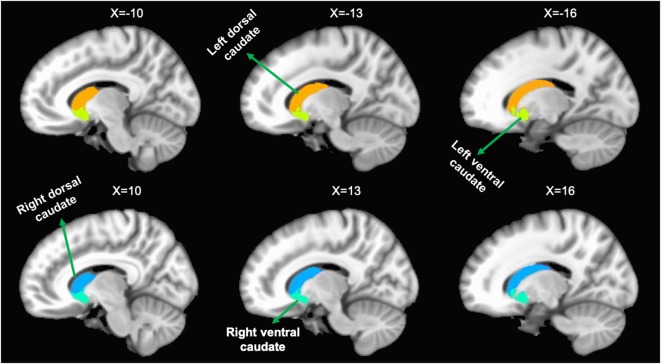
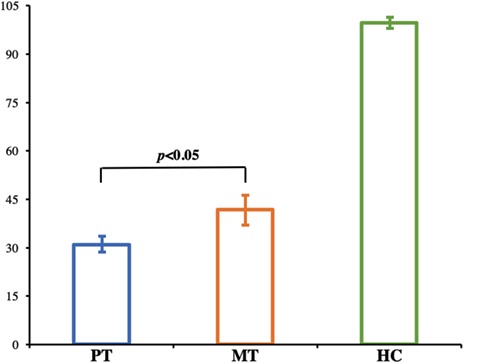
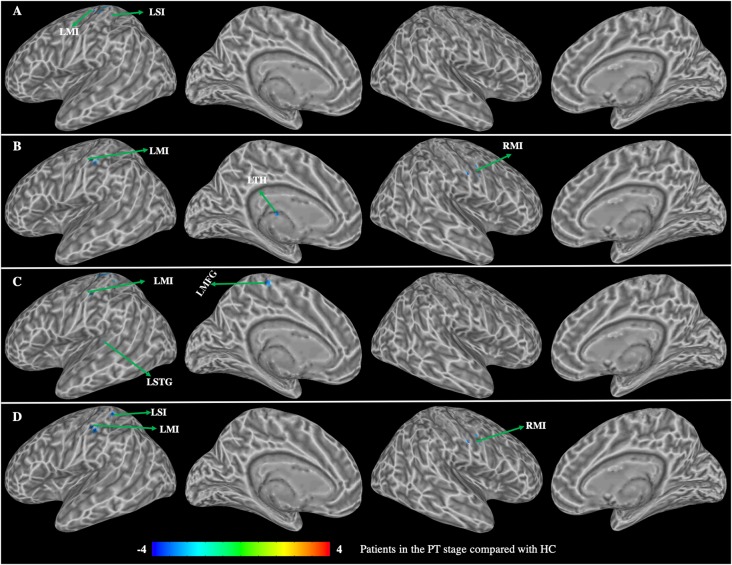
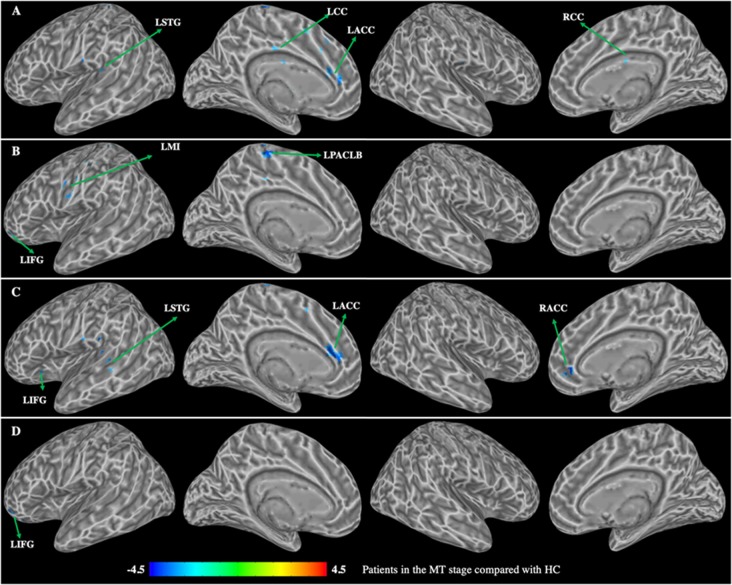
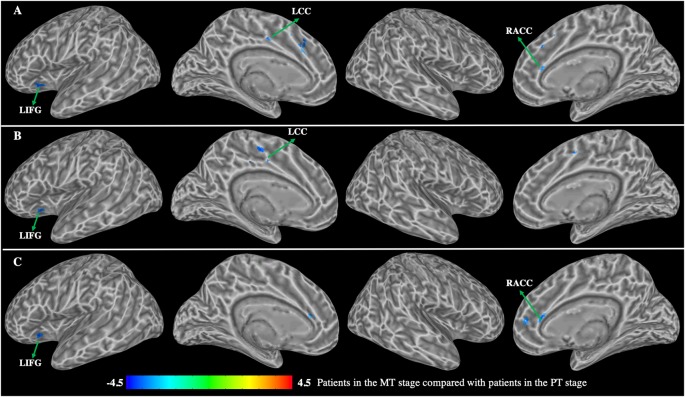
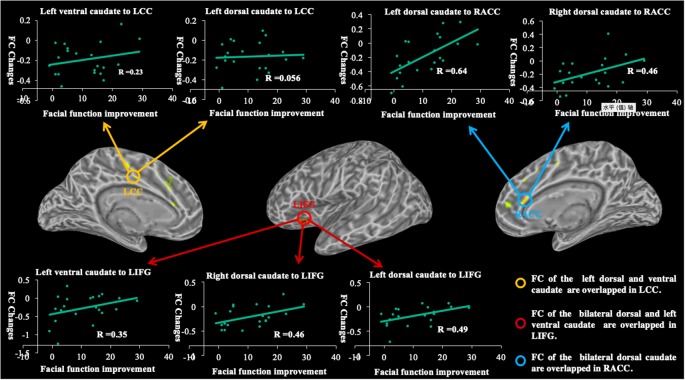
Several studies have demonstrated through resting-state functional magnetic resonance imaging (fMRI) that functional connectivity changes are important in the recovery from Bell's palsy (BP); however, these studies have only focused on the cortico-cortical connectivity. It is unclear how corticostriatal connectivity relates to the recovery process of patients with BP. In the present study, we evaluated the relationship between longitudinal changes of caudate-based functional connectivity and longitudinal changes of facial performance in patients with intractable BP. Twenty-one patients with intractable BP underwent resting-state fMRI as well as facial behavioral assessments prior to treatment (PT) and at the middle stage of treatment (MT); and 21 age- and sex-matched healthy controls (HC) were recruited and received the same protocol. The caudate was divided into dorsal and ventral sub-regions and separate functional connectivity was calculated. Compared with HC, patients with intractable BP at the PT stage showed decreased functional connectivity of both the dorsal and ventral caudate mainly distributed in the somatosensory network, including the bilateral precentral gyrus (MI), left postcentral gyrus, media frontal gyrus, and superior temporal gyrus (STG). Alternatively, patients in the MT stage showed decreased functional connectivity primarily distributed in the executive network and somatosensory network, including the bilateral cingulate cortex (CC), left anterior cingulate cortex (LACC), inferior prefrontal gyrus (IFG), MI, STG, and paracentral lobe. The longitudinal changes in functional connectivity of both the dorsal and ventral caudate were mainly observed in the executive network, including the right ACC, left CC, and IFG. Functional connectivity changes in the right ACC and left IFG were significantly correlated with changes in facial behavioral performance. These findings indicated that corticostriatal connectivity changes are associated with recovery from BP.
Keywords: Bell’s palsy; caudate; functional connectivity; functional magnetic resonance imaging; longitudinal changes.
Copyright © 2019 Hu, Kan, Kan, Li, Yuan, Xu, Wang, Wang, Bao, Shen and Wu.
Figures
Similar articles
-
Differences in functional brain alterations driven by right or left facial nerve efferent dysfunction: Evidence from early Bell's palsy.Quant Imaging Med Surg. 2019 Mar;9(3):427-439. doi: 10.21037/qims.2019.02.13. Quant Imaging Med Surg. 2019. PMID: 31032190 Free PMC article.
-
Longitudinal Changes of Caudate-Based Resting State Functional Connectivity in Mild Traumatic Brain Injury.Front Neurol. 2018 Jun 19;9:467. doi: 10.3389/fneur.2018.00467. eCollection 2018. Front Neurol. 2018. PMID: 29973909 Free PMC article.
-
Investigation of functional connectivity in Bell's palsy using functional magnetic resonance imaging: prospective cross-sectional study.Quant Imaging Med Surg. 2023 Jul 1;13(7):4676-4686. doi: 10.21037/qims-22-911. Epub 2023 Apr 13. Quant Imaging Med Surg. 2023. PMID: 37456292 Free PMC article.
-
Altered Brain Fraction Amplitude of Low Frequency Fluctuation at Resting State in Patients With Early Left and Right Bell's Palsy: Do They Have Differences?Front Neurosci. 2018 Nov 2;12:797. doi: 10.3389/fnins.2018.00797. eCollection 2018. Front Neurosci. 2018. PMID: 30450029 Free PMC article.
-
Increasing functional connectivity of the anterior cingulate cortex during the course of recovery from Bell's palsy.Neuroreport. 2015 Jan 7;26(1):6-12. doi: 10.1097/WNR.0000000000000295. Neuroreport. 2015. PMID: 25426823
References
LinkOut - more resources
Full Text Sources