

Impact on Health-Related Quality of Life of Video-Assisted Thoracoscopic Surgery for Lung Cancer
- PMID: 31788755
- PMCID: PMC7060150
- DOI: 10.1245/s10434-019-08090-4
Impact on Health-Related Quality of Life of Video-Assisted Thoracoscopic Surgery for Lung Cancer
Abstract
Background: Video-assisted thoracoscopic surgery (VATS) approaches are increasingly used in lung cancer surgery, but little is known about their impact on patients' health-related quality of life (HRQL). This prospective study measured recovery and HRQL in the year after VATS for non-small cell lung cancer (NSCLC) and explored the feasibility of HRQL data collection in patients undergoing VATS or open lung resection.
Patients and methods: Consecutive patients referred for surgical assessment (VATS or open surgery) for proven/suspected NSCLC completed HRQL and fatigue assessments before and 1, 3, 6 and 12 months post-surgery. Mean HRQL scores were calculated for patients who underwent VATS (segmental, wedge or lobectomy resection). Paired t-tests compared mean HRQL between baseline and expected worst (1 month), early (3 months) and longer-term (12 months) recovery time points.
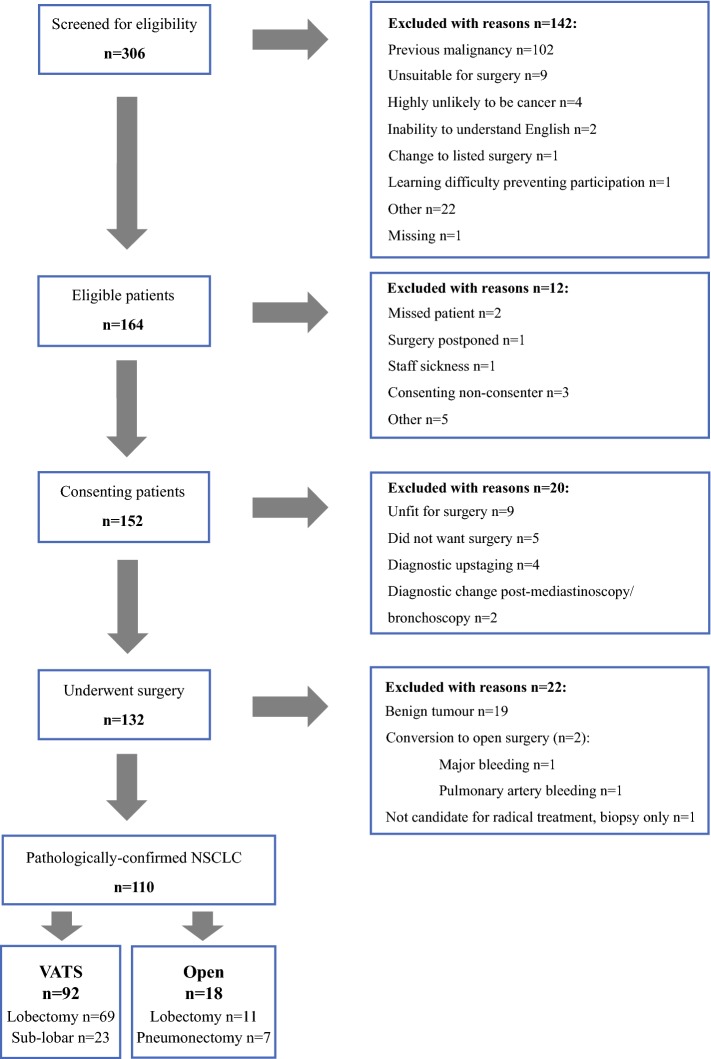
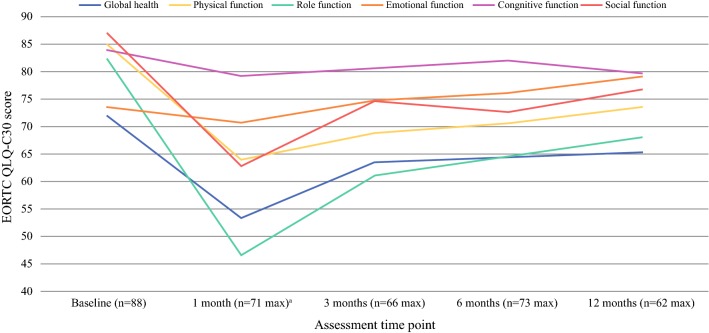
Results: A total of 92 patients received VATS, and 18 open surgery. Questionnaire response rates were high (pre-surgery 96-100%; follow-up 67-85%). Pre-surgery, VATS patients reported mostly high (good) functional health scores [(European Organisation for Research and Treatment of Cancer) EORTC function scores > 80] and low (mild) symptom scores (EORTC symptom scores < 20). One-month post-surgery, patients reported clinically and statistically significant deterioration in overall health and physical, role and social function (19-36 points), and increased fatigue, pain, dyspnoea, appetite loss and constipation [EORTC 12-26; multidimensional fatigue inventory (MFI-20) 3-5]. HRQL had not fully recovered 12 months post-surgery, with reduced physical, role and social function (10-14) and persistent fatigue and dyspnoea (EORTC 12-22; MFI-20 2.7-3.2).
Conclusions: Lung resection has a considerable detrimental impact on patients' HRQL that is not fully resolved 12 months post-surgery, despite a VATS approach.
Conflict of interest statement
DW declares grants for travel expenses from GlaxoSmithKline and grants from Above and Beyond (official charity of UHBT) during the conduct of the study. DW is a member of the NHS England Clinical Expert Group on Lung Cancer (which develops commissioning guidance for lung cancer services within NHS England), Vice Chair for the Lung Cancer Guideline Update Committee 2018 (National Institute for Health and Care Excellence) and Audit Lead for Thoracic Surgery (Society for Cardiothoracic Surgery in Britain and Ireland). DW is a member of the Cardiothoracic Specialty Specific Group, Royal College of Surgeons of Edinburgh, advising the latter on issues related to cardiothoracic surgery. DW and TB declare personal fees from AstraZeneca, Johnson and Johnson, and Medtronic outside the submitted work. TB also declares personal fees from Medela. All other authors report no conflicts of interest, financial or otherwise, with respect to this work.
Figures



References
-
- The Healthcare Quality Improvemnet Partnership . Lung cancer clinical outcomes publication 2018 (for surgical operations performed in 2016) London: Royal College of Physicians; 2018.
MeSH terms
Grants and funding
- NF-SI-0514_10114/JB holds an NIHR Senior Investigator award
- BRC-1215-20011/National Institute for Health Research (NIHR) Biomedical Research Centre at UHBT and the University of Bristol
- MR/K025643/1/Medical Research Council ConDuCT-II (Collaboration and innovation for DIfficult and Complex randomised controlled Trials In Invasive procedures) Hub for Trials Methodology Research
- 2012-13-02/Above and Beyond, the Official Charity of UHBT
- MR/K025643/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
