

Association of Patient and Visit Characteristics With Rate and Timing of Urologic Procedures for Patients Discharged From the Emergency Department With Renal Colic
- PMID: 31790565
- PMCID: PMC6902745
- DOI: 10.1001/jamanetworkopen.2019.16454
Association of Patient and Visit Characteristics With Rate and Timing of Urologic Procedures for Patients Discharged From the Emergency Department With Renal Colic
Abstract
Importance: Little is known about the timing of urologic interventions in patients with renal colic discharged from the emergency department. Understanding patients' likelihood of a subsequent urologic intervention could inform decision-making in this population.
Objectives: To examine the rate and timing of urologic procedures performed after an emergency department visit for renal colic and the factors associated with receipt of an intervention.
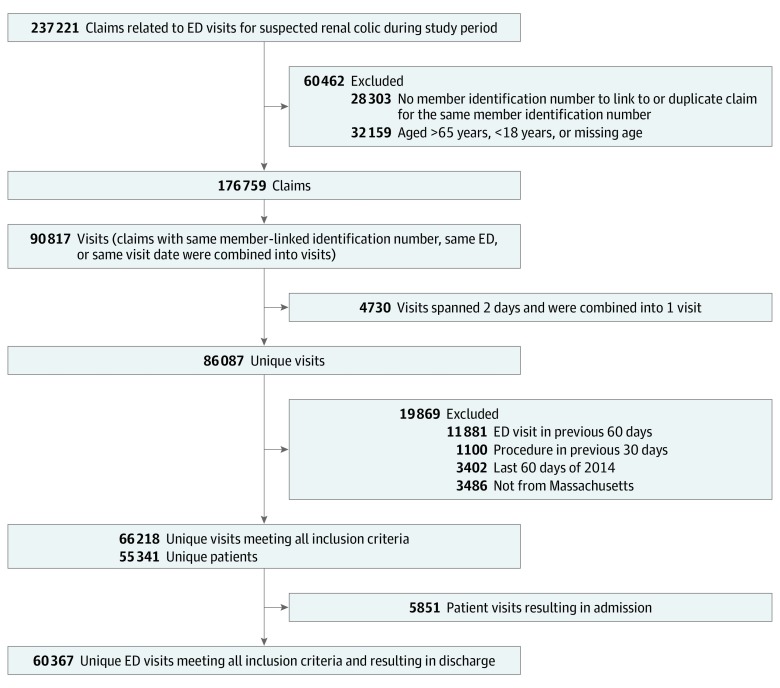
Design, setting, and participants: This retrospective cohort study used the Massachusetts All Payers Claims Database to identify patients 18 to 64 years of age who were seen in a Massachusetts emergency department for renal colic from January 1, 2011, to October 31, 2014, Patients were identified via International Classification of Diseases, Ninth Revision codes, and all medical care was linked, enabling identification of subsequent health care use. Data analysis was performed from January 1, 2017, to December 31, 2018.
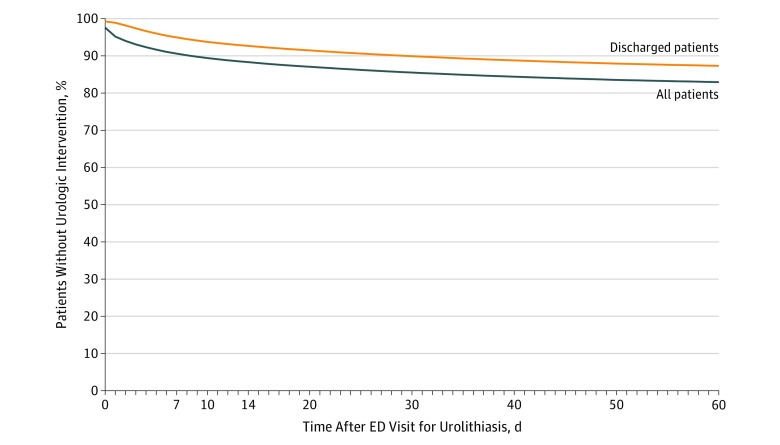
Main outcomes and measures: The main outcome was receipt of urologic procedure within 60 days. Secondary outcomes included rates of return emergency department visit and urologic and primary care follow-up.
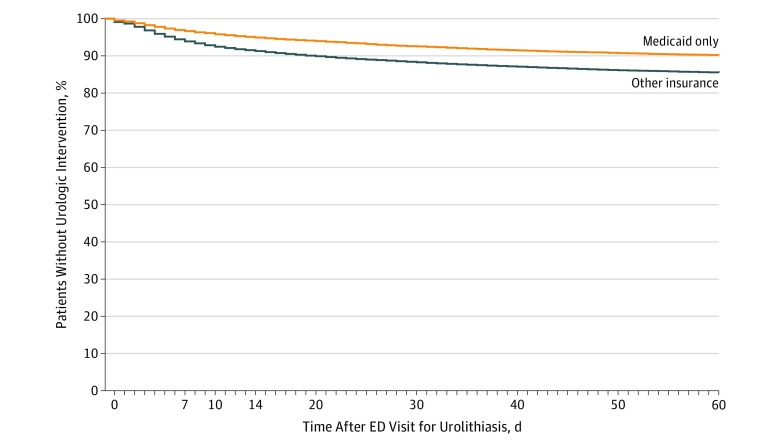
Results: A total of 66 218 unique index visits by 55 314 patients (mean [SD] age, 42.6 [12.4] years; 33 590 [50.7%] female; 25 411 [38.4%] Medicaid insured) were included in the study. A total of 5851 patients (8.8%) had visits resulting in admission at the index encounter, and 1774 (2.7%) had visits resulting in a urologic procedure during that admission. Of the 60 367 patient visits resulting in discharge from the emergency department, 3018 (5.0%) led to a urologic procedure within 7 days, 4407 (7.3%) within 14 days, 5916 (9.8%) within 28 days, and 7667 (12.7%) within 60 days. A total of 3226 visits (5.3%) led to a subsequent emergency department visit within 7 days and 6792 (11.3%) within 60 days. For the entire cohort (admitted and discharged patients), 39 189 (59.2%) had contact with a urologist or primary care practitioner within 60 days. Having Medicaid-only insurance was associated with lower rates of urologic procedures (odds ratio, 0.70; 95% CI, 0.66-0.74) and urologic follow-up (5.6% vs 8.8%; P < .001) and higher rates of primary care follow-up (59.2% vs 47.2%; P < .001) compared with patients with all other insurance types.
Conclusions and relevance: In this cohort study, most adult patients younger than 65 years who were discharged from the emergency department with a diagnosis of renal colic did not undergo a procedure or see a urologist within 60 days. This finding has implications for both the emergency department and outpatient treatment of these patients.
Conflict of interest statement
Figures
References
-
- Schoenfeld EM, Pekow PS, Shieh M-S, Scales CD Jr, Lagu T, Lindenauer PK. The diagnosis and management of patients with renal colic across a sample of us hospitals: high CT utilization despite low rates of admission and inpatient urologic intervention. PLoS One. 2017;12(1):e0169160. doi: 10.1371/journal.pone.0169160 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
