Ultrasound-based clinical profiles for predicting the risk of intradialytic hypotension in critically ill patients on intermittent dialysis: a prospective observational study
- PMID: 31791373
- PMCID: PMC6889608
- DOI: 10.1186/s13054-019-2668-2
Ultrasound-based clinical profiles for predicting the risk of intradialytic hypotension in critically ill patients on intermittent dialysis: a prospective observational study
Abstract
Background: Intradialytic hypotension, a complication of intermittent hemodialysis, decreases the efficacy of dialysis and increases long-term mortality. This study was aimed to determine whether different predialysis ultrasound cardiopulmonary profiles could predict intradialytic hypotension.
Methods: This prospective observational single-center study was performed in 248 critically ill patients with acute kidney injury undergoing intermittent hemodialysis. Immediately before hemodialysis, vena cava collapsibility was measured by vena cava ultrasound and pulmonary congestion by lung ultrasound. Factors predicting intradialytic hypotension were identified by multiple logistic regression analysis.
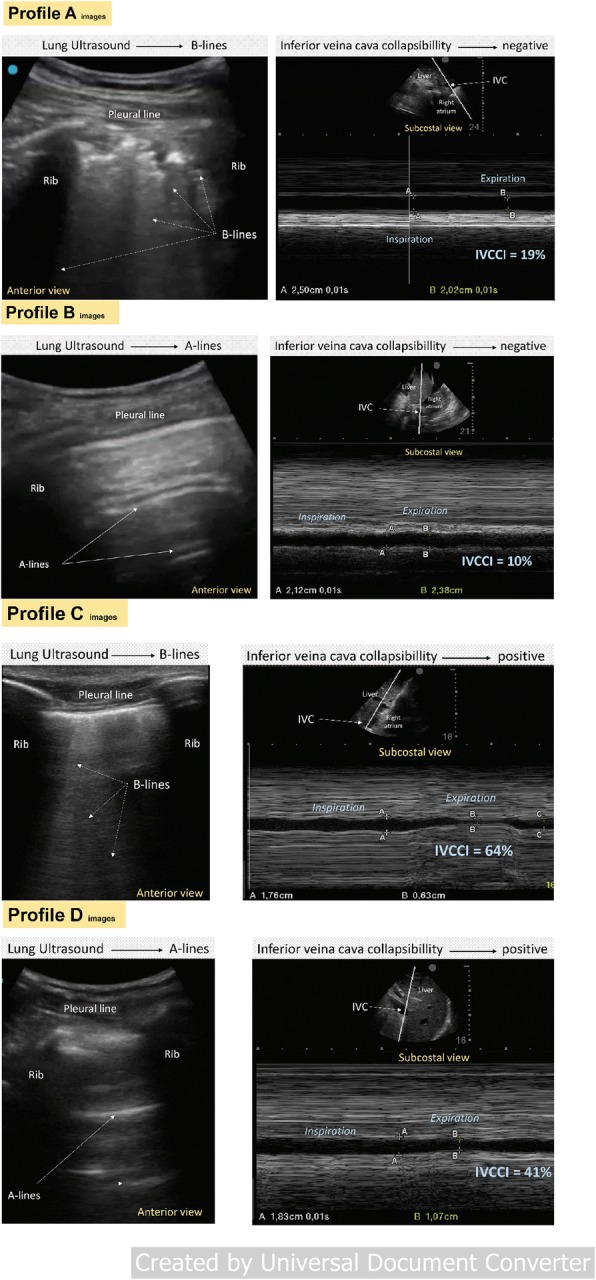
Results: Intradialytic hypotension was observed in 31.9% (n = 79) of the patients, interruption of dialysis because of intradialytic hypotension occurred in 6.8% (n = 31) of the sessions, and overall 28-day mortality was 20.1% (n = 50). Patients were classified in four ultrasound profiles: (A) 108 with B lines > 14 and vena cava collapsibility > 11.5 mm m-2, (B) 38 with B lines < 14 and vena cava collapsibility ≤ 11.5 mm m-2, (C) 36 with B lines > 14 and vena cava collapsibility Di ≤ 11.5 mm m-2, and (D) 66 with B lines < 14 and vena cava collapsibility > 11.5 mm m-2. There was an increased risk of intradialytic hypotension in patients receiving norepinephrine (odds ratios = 15, p = 0.001) and with profiles B (odds ratios = 12, p = 0.001) and C (odds ratios = 17, p = 0.001).
Conclusion: In critically ill patients on intermittent hemodialysis, the absence of hypervolemia as assessed by lung and vena cava ultrasound predisposes to intradialytic hypotension and suggests alternative techniques of hemodialysis to provide better hemodynamic stability.
Keywords: Acute kidney injury; Critically ill patients; Dialysis; Hypotension; Profiles; Ultrasound.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures