

Mechanical ventilation in patients with acute ischaemic stroke: from pathophysiology to clinical practice
- PMID: 31791375
- PMCID: PMC6889568
- DOI: 10.1186/s13054-019-2662-8
Mechanical ventilation in patients with acute ischaemic stroke: from pathophysiology to clinical practice
Abstract
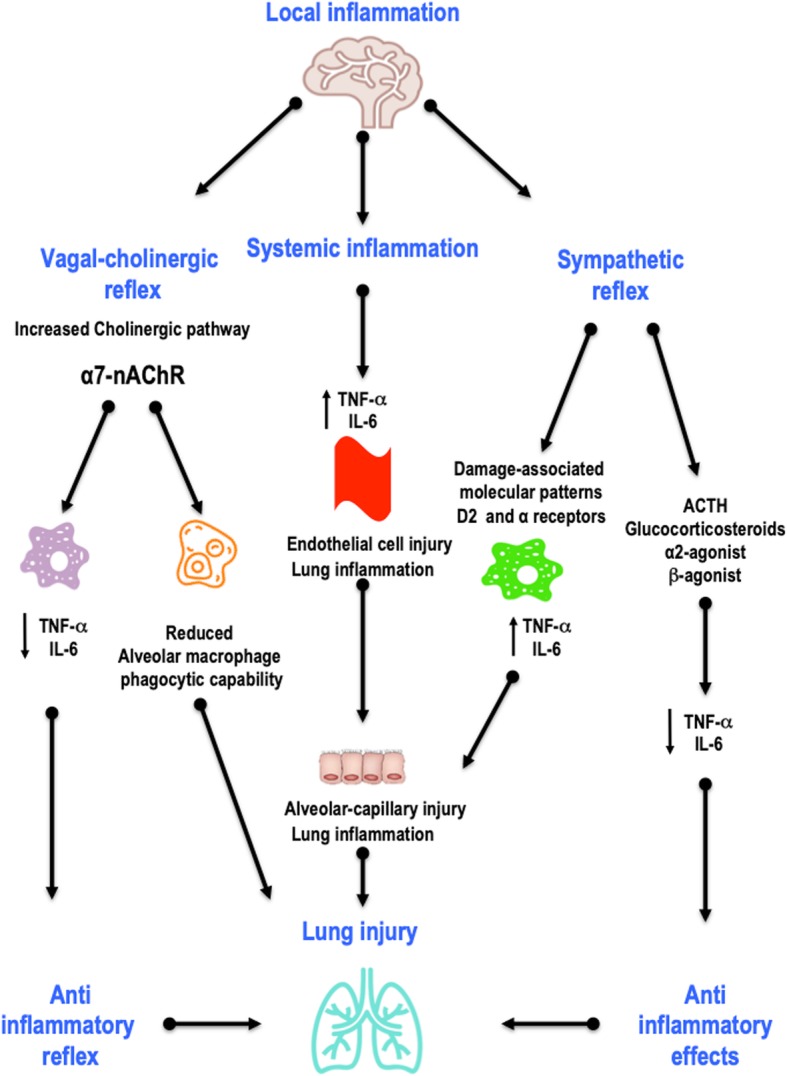
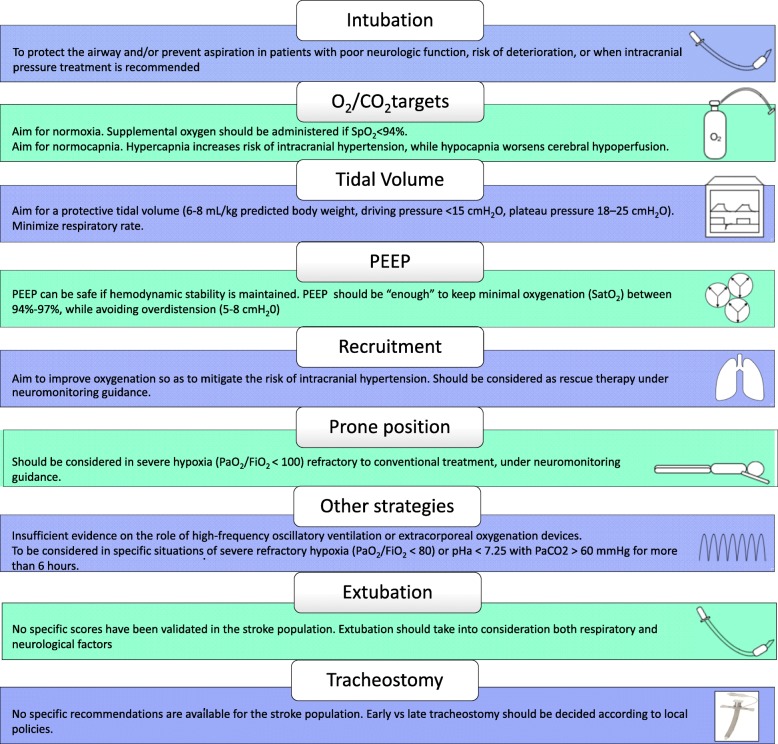
Most patients with ischaemic stroke are managed on the ward or in specialty stroke units, but a significant number requires higher-acuity care and, consequently, admission to the intensive care unit. Mechanical ventilation is frequently performed in these patients due to swallowing dysfunction and airway or respiratory system compromise. Experimental studies have focused on stroke-induced immunosuppression and brain-lung crosstalk, leading to increased pulmonary damage and inflammation, as well as reduced alveolar macrophage phagocytic capability, which may increase the risk of infection. Pulmonary complications, such as respiratory failure, pneumonia, pleural effusions, acute respiratory distress syndrome, lung oedema, and pulmonary embolism from venous thromboembolism, are common and found to be among the major causes of death in this group of patients. Furthermore, over the past two decades, tracheostomy use has increased among stroke patients, who can have unique indications for this procedure-depending on the location and type of stroke-when compared to the general population. However, the optimal mechanical ventilator strategy remains unclear in this population. Although a high tidal volume (VT) strategy has been used for many years, the latest evidence suggests that a protective ventilatory strategy (VT = 6-8 mL/kg predicted body weight, positive end-expiratory pressure and rescue recruitment manoeuvres) may also have a role in brain-damaged patients, including those with stroke. The aim of this narrative review is to explore the pathophysiology of brain-lung interactions after acute ischaemic stroke and the management of mechanical ventilation in these patients.
Keywords: Brain injury; Brain-lung crosstalk; Intensive care unit; Mechanical ventilation; Stroke.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Comment in
-
Mechanical ventilation and neurocritical patients: is there a role for anti-neuroinflammatory therapies?Crit Care. 2020 Jan 22;24(1):22. doi: 10.1186/s13054-020-2737-6. Crit Care. 2020. PMID: 31969192 Free PMC article. No abstract available.
-
Diaphragmatic dysfunction in patients with acute ischemic stroke and mechanical ventilation.Crit Care. 2020 Apr 2;24(1):127. doi: 10.1186/s13054-020-02843-4. Crit Care. 2020. PMID: 32241280 Free PMC article. No abstract available.
-
Mechanical ventilation in patients with acute ischemic stroke: from pathophysiology to clinical practice.Crit Care. 2020 Apr 7;24(1):139. doi: 10.1186/s13054-020-2806-x. Crit Care. 2020. PMID: 32264942 Free PMC article. No abstract available.
References
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet Globl Health. 2013;1:e259–e281. doi: 10.1016/S2214-109X(13)70089-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
