

BioSphincters to treat Fecal Incontinence in Nonhuman Primates
- PMID: 31792260
- PMCID: PMC6888838
- DOI: 10.1038/s41598-019-54440-3
BioSphincters to treat Fecal Incontinence in Nonhuman Primates
Abstract
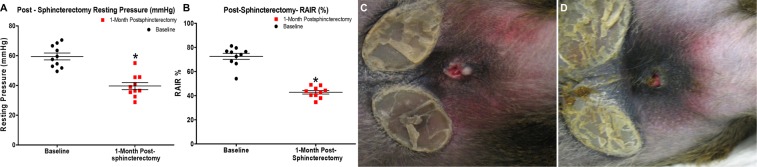
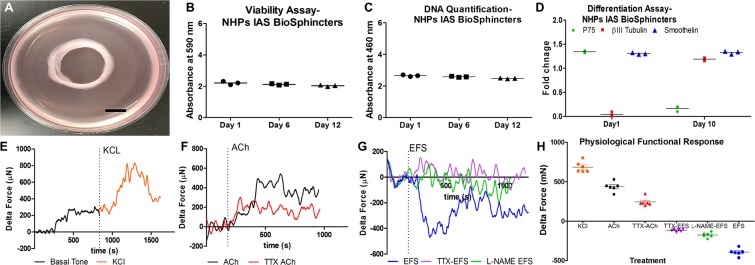
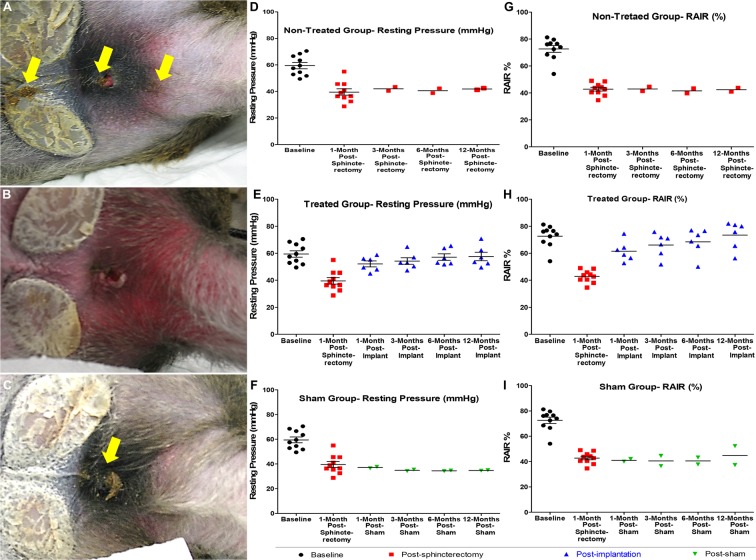
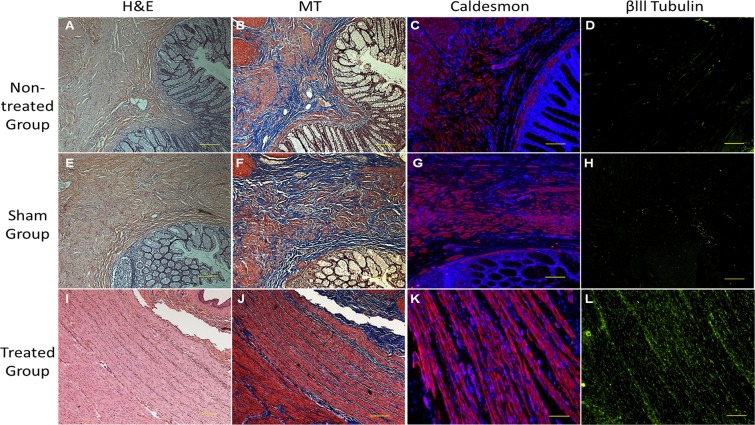
Loss of anorectal resting pressure due to internal anal sphincter (IAS) dysfunctionality causes uncontrolled fecal soiling and leads to passive fecal incontinence (FI). The study is focused on immediate and long-term safety and potential efficacy of bioengineered IAS BioSphincters to treat passive FI in a clinically relevant large animal model of passive FI. Passive FI was successfully developed in Non-Human Primates (NHPs) model. The implantation of autologous intrinsically innervated functional constructs resolved the fecal soiling, restored the resting pressure and Recto Anal Inhibitory Reflex (RAIR) within 1-month. These results were sustained with time, and efficacy was preserved up to 12-months. The histological studies validated manometric results with the regeneration of a well-organized neuro-muscular population in IAS. The control groups (non-treated and sham) remained affected by poor anal hygiene, lower resting pressure, and reduced RAIR throughout the study. The pathological assessment of implants, blood, and the vital organs confirmed biocompatibility without any adverse effect after implantation. This regenerative approach of implanting intrinsically innervated IAS BioSphincters has the potential to offer a better quality of life to the patients suffering from FI.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Bharucha AEA, et al. Epidemiology, pathophysiology, and classification of fecal incontinence: State of the Science Summary for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Workshop. Am. J. Gastroenterol. 2015;110:127–136. doi: 10.1038/ajg.2014.396. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
