

Added value of 18F-FDG-PET/CT and cardiac CTA in suspected transcatheter aortic valve endocarditis
- PMID: 31792918
- PMCID: PMC8648682
- DOI: 10.1007/s12350-019-01963-x
Added value of 18F-FDG-PET/CT and cardiac CTA in suspected transcatheter aortic valve endocarditis
Abstract
Backgrounds: Transcatheter-implanted aortic valve infective endocarditis (TAVI-IE) is difficult to diagnose when relying on the Duke Criteria. Our aim was to assess the additional diagnostic value of 18F-fluorodeoxyglucose (18F-FDG) positron emission/computed tomography (PET/CT) and cardiac computed tomography angiography (CTA) in suspected TAVI-IE.
Methods: A multicenter retrospective analysis was performed in all patients who underwent 18F-FDG-PET/CT and/or CTA with suspected TAVI-IE. Patients were first classified with Duke Criteria and after adding 18F-FDG-PET/CT and CTA, they were classified with European Society of Cardiology (ESC) criteria. The final diagnosis was determined by our Endocarditis Team based on ESC guideline recommendations.
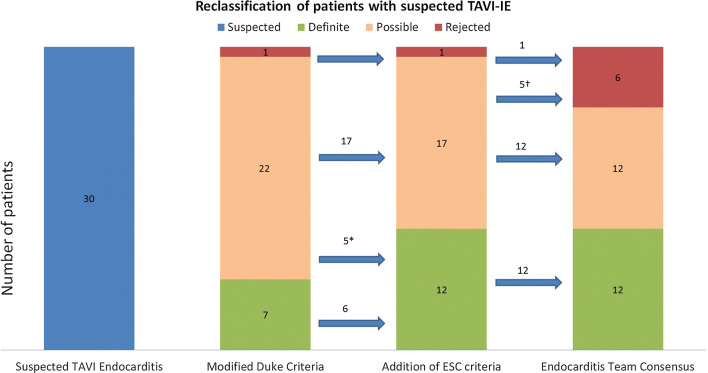
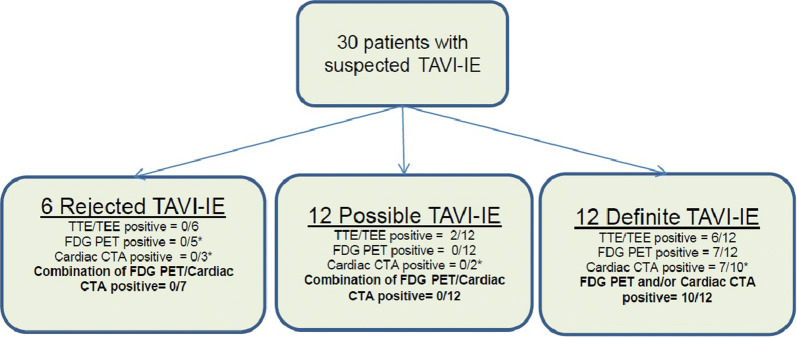
Results: Thirty patients with suspected TAVI-IE were included. 18F-FDG-PET/CT was performed in all patients and Cardiac CTA in 14/30. Using the Modified Duke Criteria, patients were classified as 3% rejected (1/30), 73% possible (22/30), and 23% definite (7/30) TAVI-IE. Adding 18F-FDG-PET/CT and CTA supported the reclassification of 10 of the 22 possible cases as "definite TAVI-IE" (5/22) or "rejected TAVI-IE" (5/22). This changed the final diagnosis to 20% rejected (6/30), 40% possible (12/30), and 40% definite (12/30) TAVI-IE.
Conclusions: Addition of 18F-FDG-PET/CT and/or CTA changed the final diagnosis in 33% of patients and proved to be a valuable diagnostic tool in patients with suspected TAVI-IE.
Keywords: CT; Infection; PET; valvular heart disease.
© 2019. The Author(s).
Figures
References
-
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J. 2015;36:3075–3128. doi: 10.1093/eurheartj/ehv319. - DOI - PubMed
-
- Saby L, Laas O, Habib G, Cammilleri S, Mancini J, Tessonnier L, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: Increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol. 2013;61:2374–2382. doi: 10.1016/j.jacc.2013.01.092. - DOI - PubMed
