

First-line R-CVP versus R-CHOP induction immunochemotherapy for indolent lymphoma with rituximab maintenance. A multicentre, phase III randomized study by the Polish Lymphoma Research Group PLRG4
- PMID: 31792945
- PMCID: PMC7154735
- DOI: 10.1111/bjh.16264
First-line R-CVP versus R-CHOP induction immunochemotherapy for indolent lymphoma with rituximab maintenance. A multicentre, phase III randomized study by the Polish Lymphoma Research Group PLRG4
Abstract
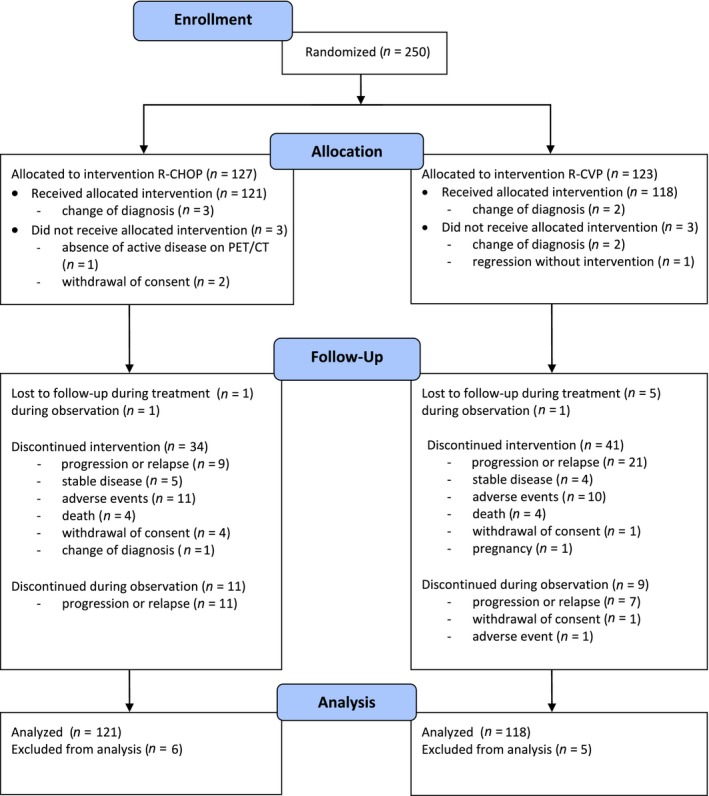
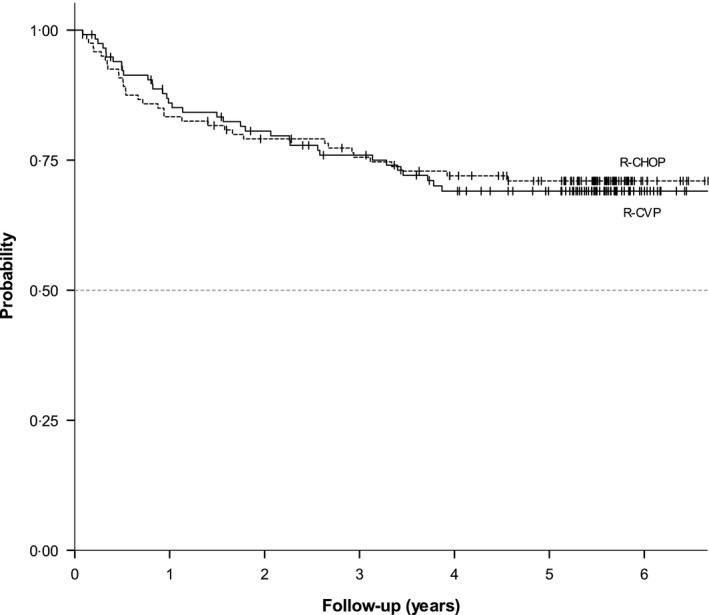
R-CVP (cyclophosphamide, vincristine, prednisone) and R-CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone + rituximab) are immunochemotherapy regimens frequently used for remission induction of indolent non-Hodgkin lymphomas (iNHLs). Rituximab maintenance (RM) significantly improves progression-free survival (PFS) in patients with complete/partial remission (CR/PR). Here we report the final results of a randomized study comparing R-CVP to R-CHOP both followed by RM. Untreated patients in need of systemic therapy with symptomatic and progressive iNHLs including follicular (FL) and marginal zone lymphoma (MZL), mucosa-associated lymphoid tissue (MALT), small lymphocytic (SLL), and lymphoplasmacytic (LPL) lymphoma were eligible. Patients were randomized to receive R-CVP or R-CHOP for eight cycles or until complete response (CR). All patients with CR/PR (partial response) received RM 375 mg/m2 q 2 months for 12 cycles. Primary endpoint was event-free survival (EFS). Two-hundred and fifty patients [FL 42%, MZL/MALT 38%, LPL/ Waldenström Macroglobulinaemia (WM) 11%, SLL 9%] were enrolled and randomized (R-CHOP: 127, R-CVP: 123). Median age was 56 years (21-85), 44% were male, 90% were in stage III-IV, 43% of FL patients had a Follicular Lymphoma International Prognostic Index (FLIPI) score ≥3, and 33·4% of all patients had an IPI score ≥3. At the end of induction treatment, the CR/PR rate was 43·6/50·9% and 36·3/60·8% in the R-CHOP and R-CVP groups (P = 0·218) respectively. After a median follow-up of 67, 66, and 70 months, five-year EFS was 61% vs. 56% (not significant), progression-free survival (PFS) was 71% vs. 69% (not significant) and overall survival (OS) was 84% vs. 89% in the R-CHOP vs. the R-CVP arm respectively. Grade III/IV adverse events (65 vs. 22) occurred in 40 (33·1%) and 18 (15·3%) patients, P = 0·001; neutropenia in 16 (11·6%) and 4 (3·4%) patients, P = 0·017; infection in 14 (10·7%) and 3 (2·5%) patients,; P = 0·011; and a second neoplasm in three versus seven patients., in the R-CHOP and the R-CVP groups respectively. This multicentre randomized study with >five-year follow-up shows similar outcome in patients with indolent lymphoma in need of systemic therapy treated with R-CVP or R-CHOP immunochemotherapy and rituximab maintenance in both arms. The minor toxicity of the R-CVP regimen makes it a reasonable choice for induction treatment, leaving other active agents like doxorubicin or bendamustin for second-line therapy.
Keywords: first-line induction immunochemotherapy; indolent lymphoma; rituximab maintenance.
© 2019 The Authors. British Journal of Haematology published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
JW — Advisory role: Roche, Celgene, Takeda, Janssen‐Cilag, Servier, Amgen, BMS, Abbvie, Novartis, Gilead; research funding: Roche, GSK/Novartis, Takeda, Janssen‐Cilag; lecture honoraria: Roche, Celgene, Takeda, Janssen‐Cilag, Servier; Amgen; conference travel support: Roche. EPK — lecture honoraria: Roche, Takeda, Servier; conference travel support: Roche, Takeda, Celgene. GR — conference travel support: Roche, Takeda, Servier. TS — conference travel support: Roche. JMZ — lecture honoraria, conference travel support, research funding: Roche; advisory role: Takeda, Abbvie; lecture honoraria: Janssen‐Cilag. EKW — lecture honoraria: Roche; conference travel support: Roche. JRJ — lecture honoraria: Roche; conference travel support: Roche. ADI — conference travel support: Roche, Sanofi, Amgen. AD — advisory role: Roche, Celgene, Amgen; lecture honoraria: Roche, Celgene, Amgen, GSK/Novartis, Servier. WJ — research funding: Roche, Celtrion, Sandoz Novartis, Janssen, Acerta, Merck, Beigene, TG therapeutics, Gilead, Celgene; advisory role: Sandoz Novartis, Janssen, Acerta, Abbvie, Servier. WM, AB, AG, AW, DZC, WKP, AT, BG, MJJ, AB, WH, AP, AR, AH, BSH — none declared.
Figures

References
-
- Bachy, E. , Houot, R. , Morschhauser, F. , Sonet, A. , Brice, P. , Belhadj, K. , Cartron, G. , Audhuy, B. , Ferme, C. , Feugier, P. , Sebban, C. , Delwail, V. , Maisonneuve, H. , Le Gouill, S. , Lefort, S. , Brousse, N. , Foussard, C. & Salles, G. (2013) Long‐term follow up of the FL2000 study comparing CHVP‐interferon to CHVP‐interferon plus rituximab in follicular lymphoma. Haematologica, 98, 1107–1114. - PMC - PubMed
-
- Cheson, B.D. , Horning, S.J. , Coiffier, B. , Shipp, M.A. , Fisher, R.I. , Connors, J.M. , Lister, T.A. , Vose, J. , Grillo‐López, A. , Hagenbeek, A. & Cabanillas, F. (1999) Report of an international workshop to standardize response criteria for non‐Hodgkin's lymphomas. NCI Sponsored International Working Group. Journal of Clinical Oncology, 17, 1244. - PubMed
-
- Cheson, B.D. , Pfistner, B. , Juweid, M.E. , Gascoyne, R.D. , Specht, L. , Horning, S.J. , Coiffier, B. , Fisher, R.I. , Hagenbeek, A. , Zucca, E. & Rosen, S.T. (2007) Revised response criteria for malignant lymphoma. Journal of Clinical Oncology, 25, 579–586. - PubMed
-
- Federico, M. , Luminari, S. , Dondi, A. , Tucci, A. , Vitolo, U. , Rigacci, L. , Di Raimondo, F. , Carella, A.M. , Pulsoni, A. , Merli, F. & Arcaini, L. (2013) R‐CVP versus R‐CHOP versus R‐FM for the initial treatment of patients with advanced‐stage follicular lymphoma: results of the FOLL05 trial conducted by the Fondazione Italiana Linfomi. Journal of Clinical Oncology, 31, 1506–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
