

Preoperative Risk and the Association between Hypotension and Postoperative Acute Kidney Injury
- PMID: 31794513
- PMCID: PMC7015776
- DOI: 10.1097/ALN.0000000000003063
Preoperative Risk and the Association between Hypotension and Postoperative Acute Kidney Injury
Erratum in
-
Preoperative Risk and the Association between Hypotension and Postoperative Acute Kidney Injury: Erratum.Anesthesiology. 2020 Apr;132(4):937. doi: 10.1097/ALN.0000000000003144. Anesthesiology. 2020. PMID: 31917705 No abstract available.
Abstract
Background: Despite the significant healthcare impact of acute kidney injury, little is known regarding prevention. Single-center data have implicated hypotension in developing postoperative acute kidney injury. The generalizability of this finding and the interaction between hypotension and baseline patient disease burden remain unknown. The authors sought to determine whether the association between intraoperative hypotension and acute kidney injury varies by preoperative risk.
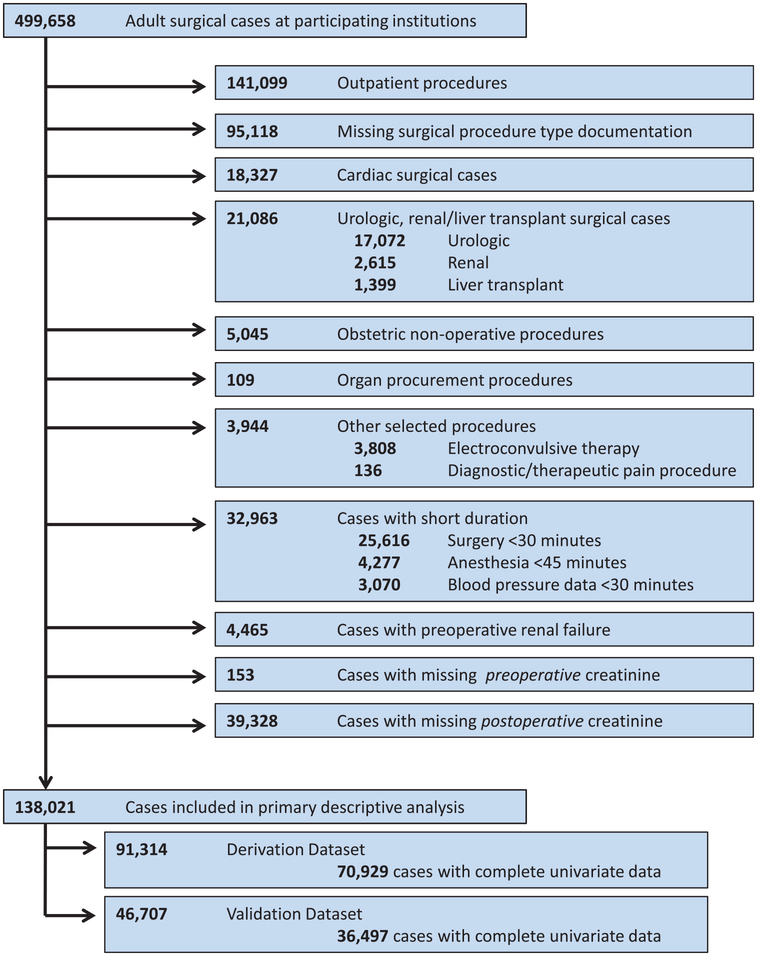
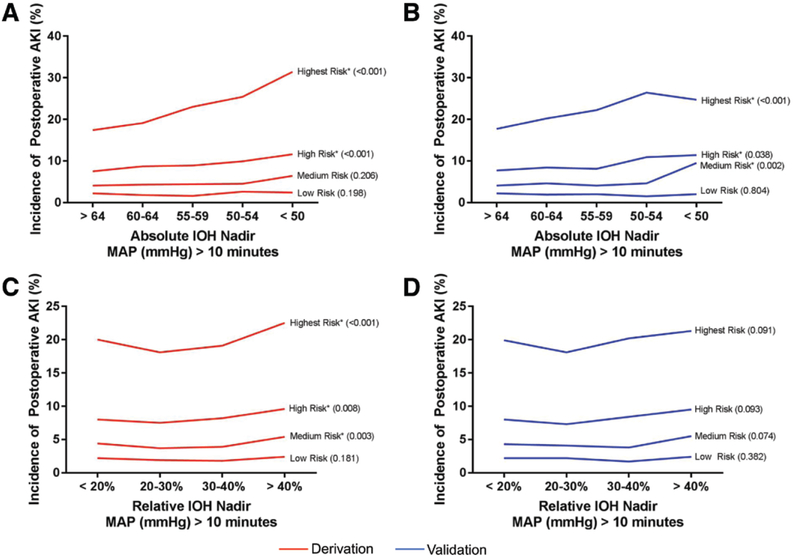
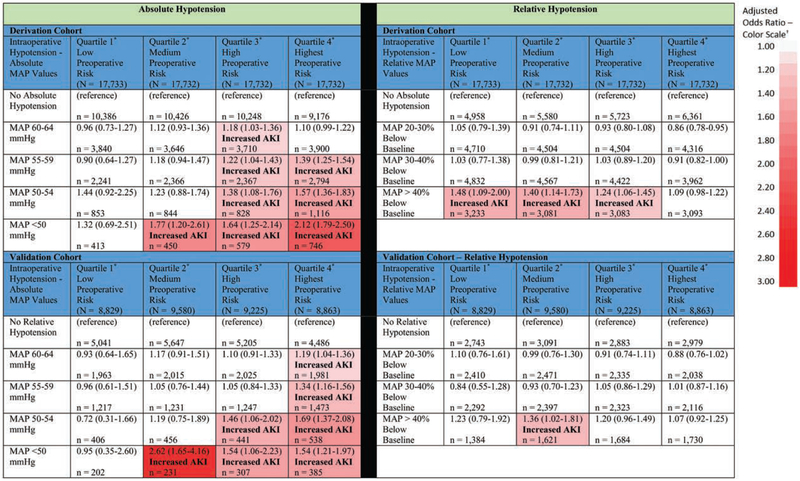
Methods: Major noncardiac surgical procedures performed on adult patients across eight hospitals between 2008 and 2015 were reviewed. Derivation and validation cohorts were used, and cases were stratified into preoperative risk quartiles based upon comorbidities and surgical procedure. After preoperative risk stratification, associations between intraoperative hypotension and acute kidney injury were analyzed. Hypotension was defined as the lowest mean arterial pressure range achieved for more than 10 min; ranges were defined as absolute (mmHg) or relative (percentage of decrease from baseline).
Results: Among 138,021 cases reviewed, 12,431 (9.0%) developed postoperative acute kidney injury. Major risk factors included anemia, estimated glomerular filtration rate, surgery type, American Society of Anesthesiologists Physical Status, and expected anesthesia duration. Using such factors and others for risk stratification, patients with low baseline risk demonstrated no associations between intraoperative hypotension and acute kidney injury. Patients with medium risk demonstrated associations between severe-range intraoperative hypotension (mean arterial pressure less than 50 mmHg) and acute kidney injury (adjusted odds ratio, 2.62; 95% CI, 1.65 to 4.16 in validation cohort). In patients with the highest risk, mild hypotension ranges (mean arterial pressure 55 to 59 mmHg) were associated with acute kidney injury (adjusted odds ratio, 1.34; 95% CI, 1.16 to 1.56). Compared with absolute hypotension, relative hypotension demonstrated weak associations with acute kidney injury not replicable in the validation cohort.
Conclusions: Adult patients undergoing noncardiac surgery demonstrate varying associations with distinct levels of hypotension when stratified by preoperative risk factors. Specific levels of absolute hypotension, but not relative hypotension, are an important independent risk factor for acute kidney injury.
Conflict of interest statement
Competing Interests
The authors declare no competing interests.
Figures
Comment in
-
Preoperative Risk, Blood Pressure, and Acute Kidney Injury.Anesthesiology. 2020 Mar;132(3):416-417. doi: 10.1097/ALN.0000000000003101. Anesthesiology. 2020. PMID: 31929330 No abstract available.
References
-
- Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T, Fu R, Azad T, Chao TE, Berry WR, Gawande AA: Estimate of the global volume of surgery in 2012: An assessment supporting improved health outcomes. Lancet 2015; 385:S11 - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB: Complications, failure to rescue, and mortality with major inpatient surgery in Medicare patients. Ann Surg 2009; 250:1029–34 - PubMed
-
- Garg AX, Kurz A, Sessler DI, Cuerden M, Robinson A, Mrkobrada M, Parikh CR, Mizera R, Jones PM, Tiboni M, Font A, Cegarra V, Gomez MF, Meyhoff CS, VanHelder T, Chan MT, Torres D, Parlow J, Clanchet Mde N, Amir M, Bidgoli SJ, Pasin L, Martinsen K, Malaga G, Myles P, Acedillo R, Roshanov PS, Walsh M, Dresser G, Kumar P, Fleischmann E, Villar JC, Painter T, Biccard B, Bergese S, Srinathan S, Cata JP Chan V, Mehra B, Wijeysundera DN, Leslie K, Forget P, Whitlock R, Yusuf S, Devereaux PJ; POISE-2 Investigators: Perioperative aspirin and clonidine and risk of acute kidney injury: A randomized clinical trial. JAMA 2014; 312:2254–64 - PubMed
-
- Biteker M, Dayan A, Tekkeşin Aİ, Can MM, Taycı İ, İlhan E, Şahin G: Incidence, risk factors, and outcomes of perioperative acute kidney injury in noncardiac and nonvascular surgery. Am J Surg 2014; 207:53–9 - PubMed
