

Effect of Single-Fraction vs Multifraction Radiotherapy on Ambulatory Status Among Patients With Spinal Canal Compression From Metastatic Cancer: The SCORAD Randomized Clinical Trial
- PMID: 31794625
- PMCID: PMC6902166
- DOI: 10.1001/jama.2019.17913
Effect of Single-Fraction vs Multifraction Radiotherapy on Ambulatory Status Among Patients With Spinal Canal Compression From Metastatic Cancer: The SCORAD Randomized Clinical Trial
Abstract
Importance: Malignant spinal canal compression, a major complication of metastatic cancer, is managed with radiotherapy to maintain mobility and relieve pain, although there is no standard radiotherapy regimen.
Objective: To evaluate whether single-fraction radiotherapy is noninferior to 5 fractions of radiotherapy.
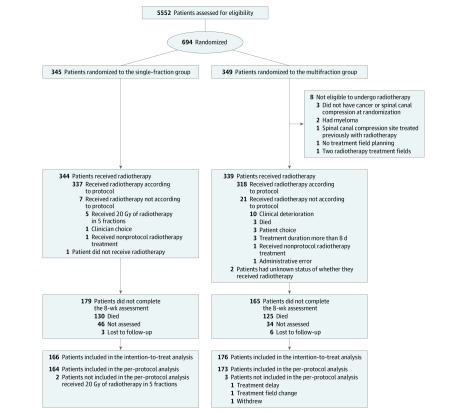
Design, setting, and participants: Multicenter noninferiority randomized clinical trial conducted in 42 UK and 5 Australian radiotherapy centers. Eligible patients (n = 686) had metastatic cancer with spinal cord or cauda equina compression, life expectancy greater than 8 weeks, and no previous radiotherapy to the same area. Patients were recruited between February 2008 and April 2016, with final follow-up in September 2017.
Interventions: Patients were randomized to receive external beam single-fraction 8-Gy radiotherapy (n = 345) or 20 Gy of radiotherapy in 5 fractions over 5 consecutive days (n = 341).
Main outcomes and measures: The primary end point was ambulatory status at week 8, based on a 4-point scale and classified as grade 1 (ambulatory without the use of aids and grade 5 of 5 muscle power) or grade 2 (ambulatory using aids or grade 4 of 5 muscle power). The noninferiority margin for the difference in ambulatory status was -11%. Secondary end points included ambulatory status at weeks 1, 4, and 12 and overall survival.
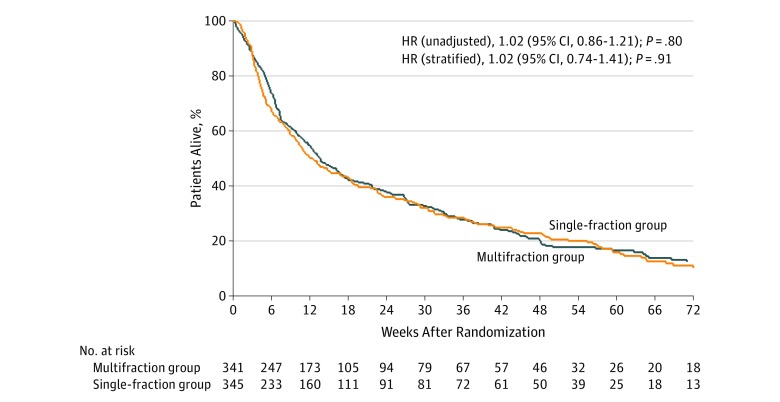
Results: Among 686 randomized patients (median [interquartile range] age, 70 [64-77] years; 503 (73%) men; 44% had prostate cancer, 19% had lung cancer, and 12% had breast cancer), 342 (49.8%) were analyzed for the primary end point (255 patients died before the 8-week assessment). Ambulatory status grade 1 or 2 at week 8 was achieved by 115 of 166 (69.3%) patients in the single-fraction group vs 128 of 176 (72.7%) in the multifraction group (difference, -3.5% [1-sided 95% CI, -11.5% to ∞]; P value for noninferiority = .06). The difference in ambulatory status grade 1 or 2 in the single-fraction vs multifraction group was -0.4% (63.9% vs 64.3%; [1-sided 95% CI, -6.9 to ∞]; P value for noninferiority = .004) at week 1, -0.7% (66.8% vs 67.6%; [1-sided 95% CI, -8.1 to ∞]; P value for noninferiority = .01) at week 4, and 4.1% (71.8% vs 67.7%; [1-sided 95% CI, -4.6 to ∞]; P value for noninferiority = .002) at week 12. Overall survival rates at 12 weeks were 50% in the single-fraction group vs 55% in the multifraction group (stratified hazard ratio, 1.02 [95% CI, 0.74-1.41]). Of the 11 other secondary end points that were analyzed, the between-group differences were not statistically significant or did not meet noninferiority criterion.
Conclusions and relevance: Among patients with malignant metastatic solid tumors and spinal canal compression, a single radiotherapy dose, compared with a multifraction dose delivered over 5 days, did not meet the criterion for noninferiority for the primary outcome (ambulatory at 8 weeks). However, the extent to which the lower bound of the CI overlapped with the noninferiority margin should be considered when interpreting the clinical importance of this finding.
Trial registration: ISRCTN Identifiers: ISRCTN97555949 and ISRCTN97108008.
Conflict of interest statement
Figures

References
-
- Metastatic spinal cord compression in adults: risk assessment, diagnosis and management. Manchester, UK: National Institute for Health and Clinical Excellence ; 2008. https://www.nice.org.uk/guidance/cg75/resources/metastatic-spinal-cord-c.... Published November 26, 2008. Accessed August 8, 2019. - PubMed
-
- Loblaw DA, Perry J, Chambers A, Laperriere NJ. Systematic review of the diagnosis and management of malignant extradural spinal cord compression: the Cancer Care Ontario Practice Guidelines Initiative’s Neuro-Oncology Disease Site Group. J Clin Oncol. 2005;23(9):2028-2037. doi:10.1200/JCO.2005.00.067 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
