

EEG time signature in Alzheimer´s disease: Functional brain networks falling apart
- PMID: 31795039
- PMCID: PMC6909352
- DOI: 10.1016/j.nicl.2019.102046
EEG time signature in Alzheimer´s disease: Functional brain networks falling apart
Abstract
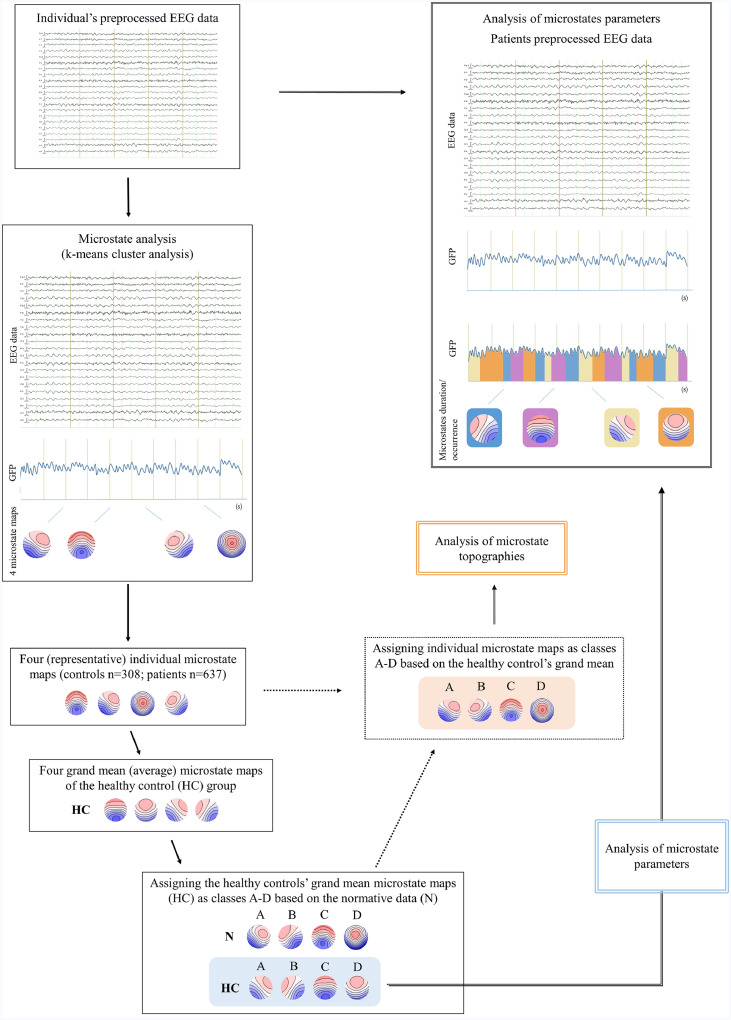
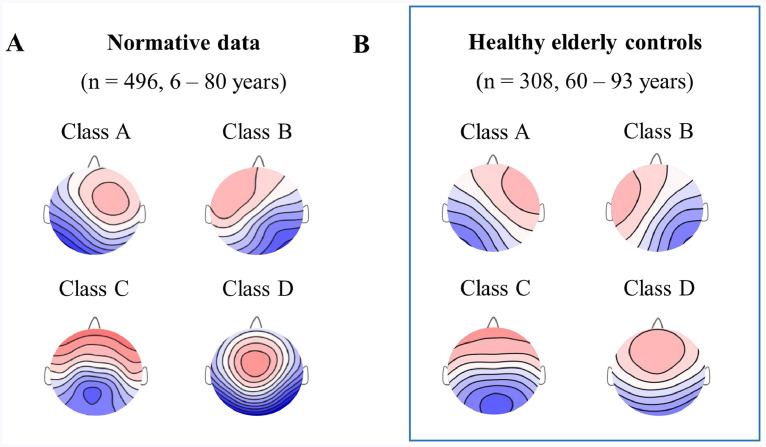
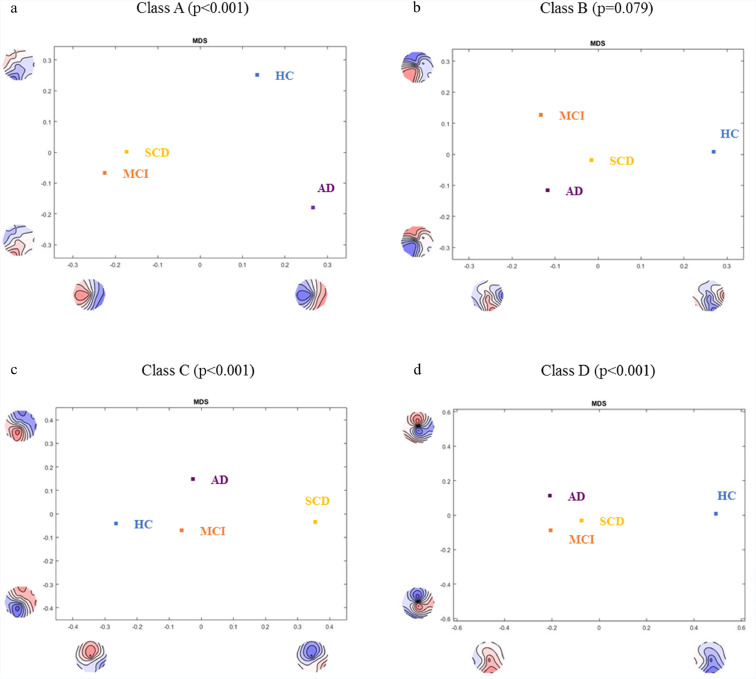
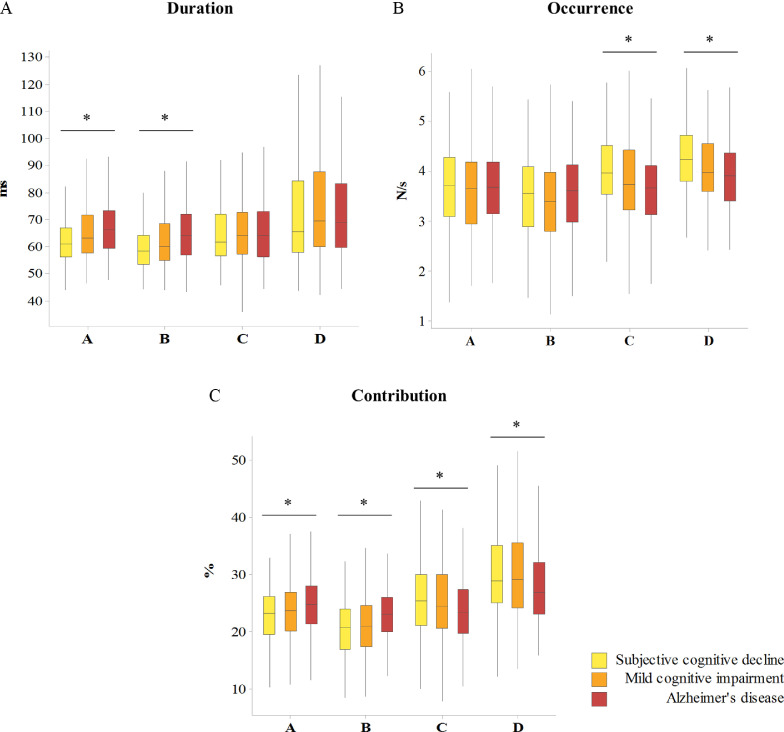
Spontaneous mental activity is characterized by dynamic alterations of discrete and stabile brain states called functional microstates that are thought to represent distinct steps of human information processing. Electroencephalography (EEG) directly reflects functioning of brain synapses with a uniquely high temporal resolution, necessary for investigation of brain network dynamics. Since synaptic dysfunction is an early event and best correlate of cognitive status and decline in patients along Alzheimer's disease (AD) continuum, EEG microstates might serve as valuable early markers of AD. The present study investigated differences in EEG microstate topographies and parameters (duration, occurrence and contribution) between a large cohort of healthy elderly (n = 308) and memory clinic patients: subjective cognitive decline (SCD, n = 210); mild cognitive impairment (MCI, n = 230) and AD (n = 197) and how they correlate to conventional cerebrospinal fluid (CSF) markers of AD. Four most representative microstate maps assigned as classes A, B (asymmetrical), C and D (symmetrical) were computed from the resting state EEGs since it has been shown previously that this is sufficient to explain most of the resting state EEG data. Statistically different topography of microstate maps were found between the controls and the patient groups for microstate classes A, C and D. Changes in the topography of microstate class C were associated with the CSF Aβ42 levels, whereas changes in the topography of class B were linked with the CSF p-tau levels. Gradient-like increase in the contribution of asymmetrical (A and B) and gradient-like decrease in the contribution of symmetrical (C and D) maps were observed with the more severe stage of cognitive impairment. Our study demonstrated extensive relationship of resting state EEG microstates topographies and parameters with the stage of cognitive impairment and AD biomarkers. Resting state EEG microstates might therefore serve as functional markers of early disruption of neurocognitive networks in patients along AD continuum.
Keywords: Alzheimer's disease; Biomarkers; Cerebrospinal fluid; Electroencephalography; Functional microstates.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bartzokis G. Age-related myelin breakdown: a developmental model of cognitive decline and Alzheimer’s disease. Neurobiol Aging. 2004;25(1):5–18. - PubMed
-
- Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat. Rev. Neurol. 2010;6(3):131–144. - PubMed
-
- Braak E., Griffing K., Arai K., Bohl J., Bratzke H., Braak H. Neuropathology of Alzheimer’s disease: what is new since A. Alzheimer? Eur Arch Psychiatry Clin Neurosci. 1999;249(3):14–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
