

Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis
- PMID: 31795171
- PMCID: PMC6956009
- DOI: 10.3390/medicina55120762
Pharmacologic and Non-Pharmacologic Interventions for HIV-Neuropathy Pain. A Systematic Review and a Meta-Analysis
Abstract
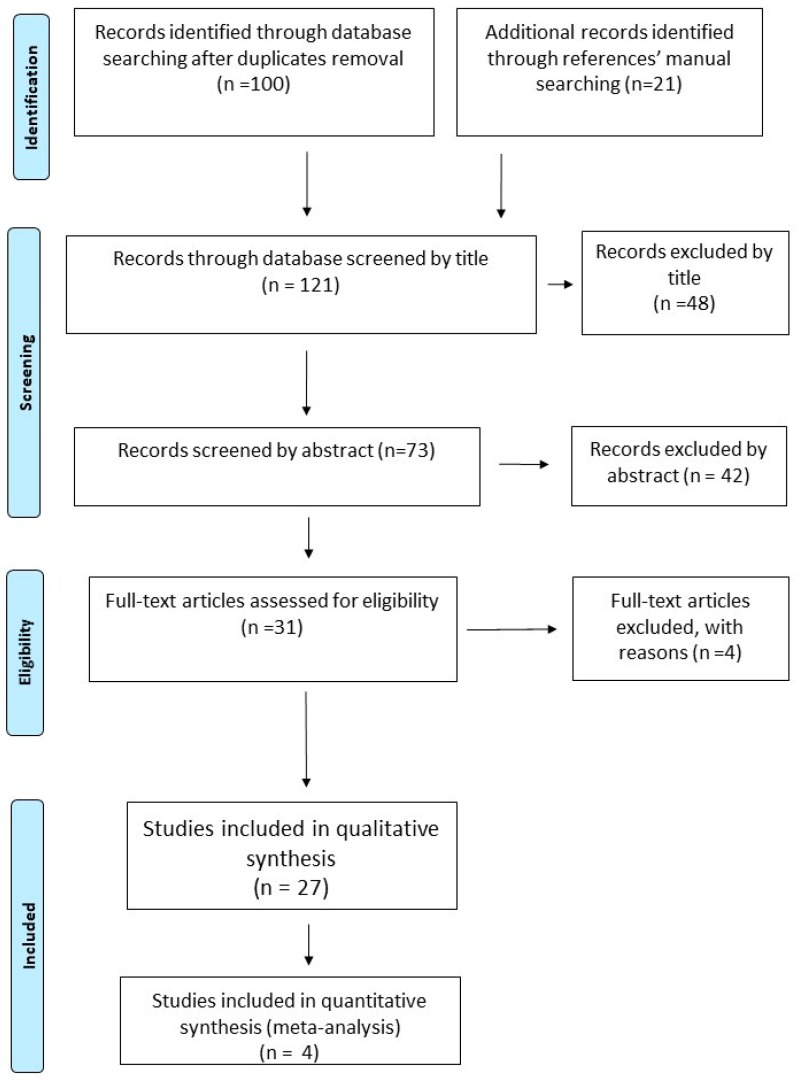
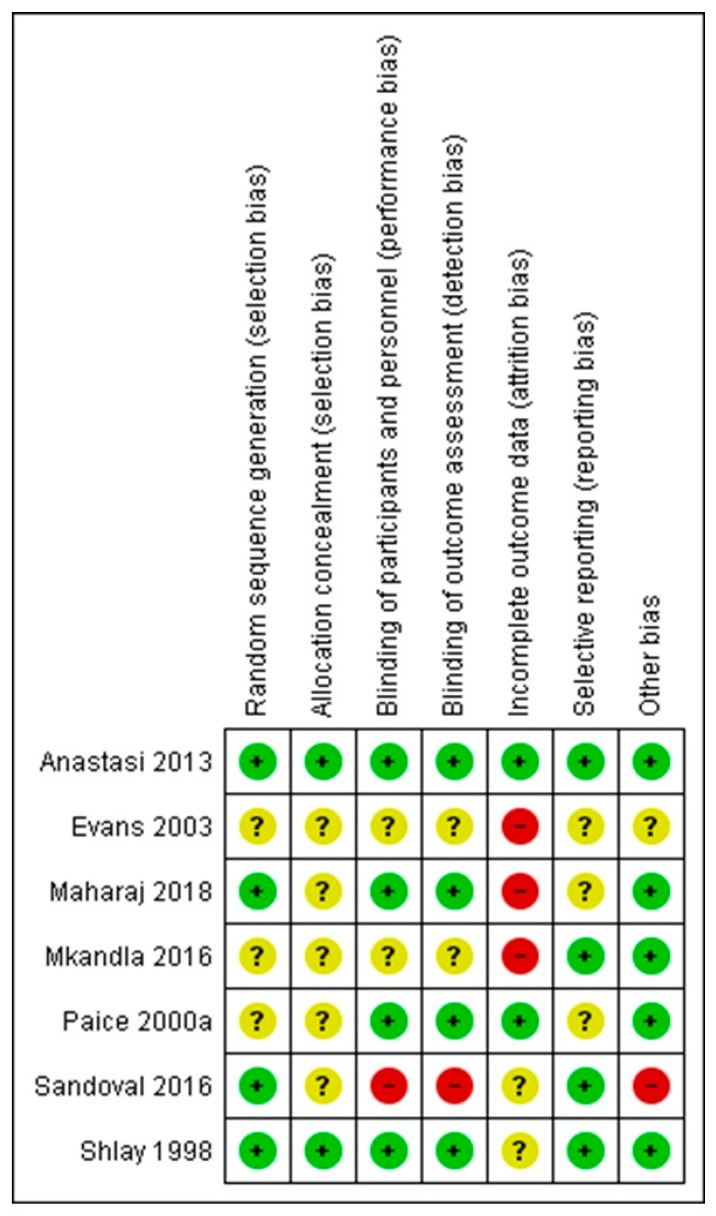
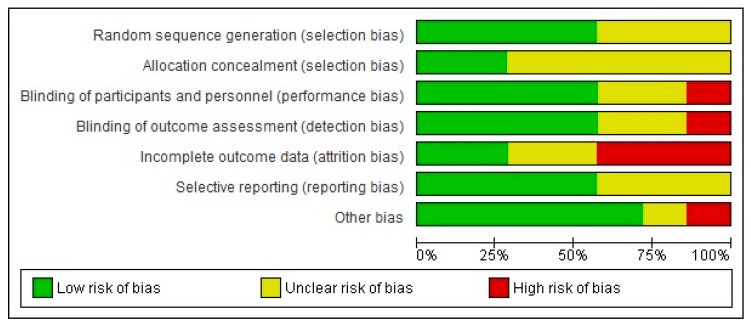
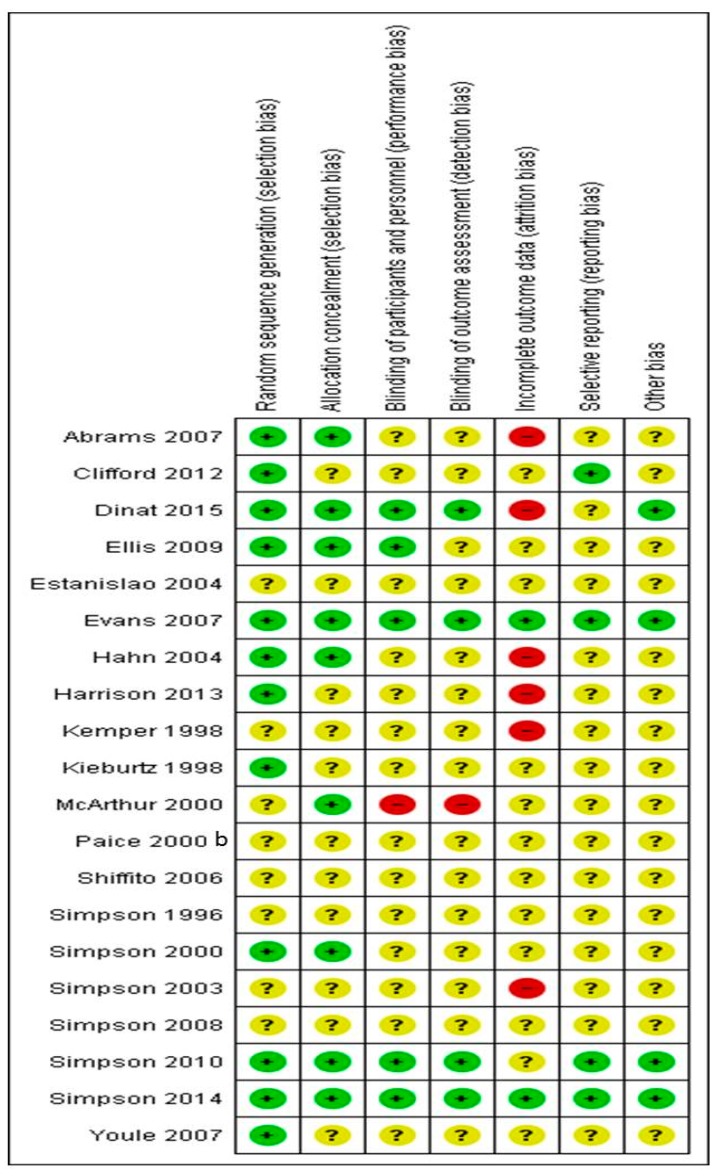
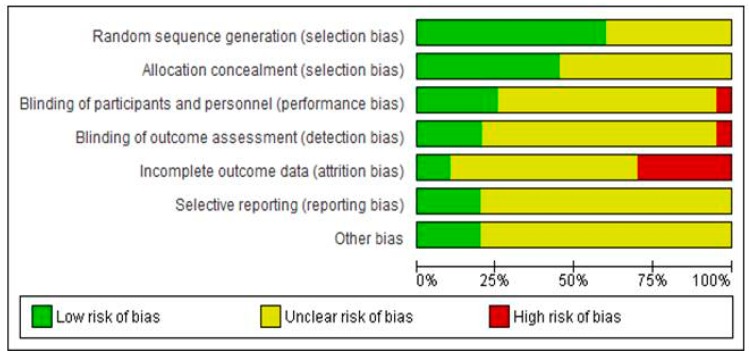
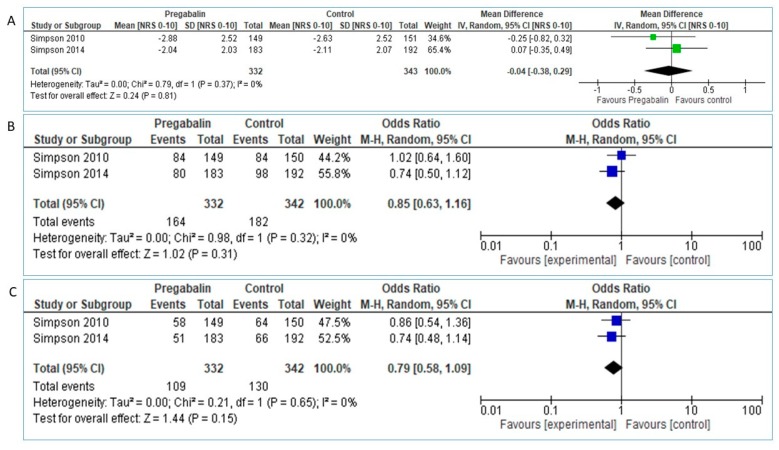
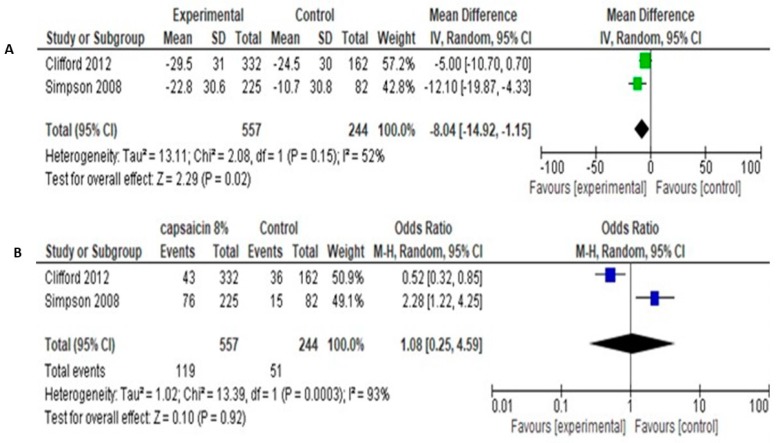
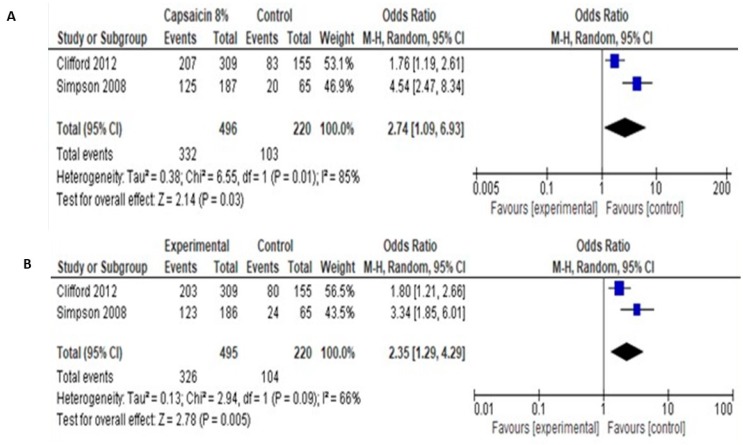
Background and Objectives: Among HIV infection symptoms, sensory neuropathy (HIV-SN) remains a main cause of suffering, with incidence varying from 13-50%. So far, numerous pharmacological and non-pharmacological treatments have been tested, although few evidence-based analgesic options are available. We conducted an up-to-date systematic review and meta-analysis of the literature in order to evaluate the efficacy and safety of pharmacologic and non-pharmacologic treatments for pain control, in patients with HIV neuropathy. Materials and Methods: We searched MEDLINE, EMBASE, Scopus/Elsevier, The Cochrane Central Register of Controlled Trials (CENTRAL), USA Clinical Trials registry, and The International Web of Science up to April 2019. All randomized controlled trials evaluating efficacy and safety of non-pharmacologic and pharmacologic therapies were included. Efficacy was defined as pain reduction during the study period. Safety was estimated from adverse events. A meta-analysis was performed whenever possible. Results: 27 randomized controlled trials (RCTs) were included for analysis (7 evaluating non pharmacologic interventions, 20 pharmacologic therapies). Non-pharmacologic studies (n = 742) involved seven different therapeutic modalities. Only Acupuncture/Moxibustion showed pain reduction over placebo, Gracely Pain Scale Mean (SD): Acu/Moxa 0.85 (0.12), placebo 1.10 (0.09), p = 0.05. Pharmacologic studies, involving 2516 patients revealed efficacy for capsaicin 8% over placebo (mean difference -8.04 [95% CI: -14.92 -1.15], smoked cannabis (where pooling data for meta-analysis was not possible) and recombinant Nerve Growth Factor. Conclusion: Despite various modalities for pain control in HIV-SN, strongest evidence exists for capsaicin 8% and smoked cannabis, although of low methodological quality. Among non-pharmacologic modalities, only Acu/Moxa gave a marginal beneficial effect in one study, possibly limited by inherent methodological flaws.
Keywords: HIV; infectious disease; neuropathy; pain.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Lichtenstein K.A., Armon C., Baron A., Moorman A.C., Wood K.C., Holmberg S.D. Modification of the incidence of drug-associated symmetrical peripheral neuropathy by host and disease factors in the HIV outpatient study cohort. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005;40:148–157. doi: 10.1086/426076. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
