

Geographic Analysis of Mobile Stroke Unit Treatment in a Dense Urban Area: The New York City METRONOME Registry
- PMID: 31795824
- PMCID: PMC6951069
- DOI: 10.1161/JAHA.119.013529
Geographic Analysis of Mobile Stroke Unit Treatment in a Dense Urban Area: The New York City METRONOME Registry
Abstract
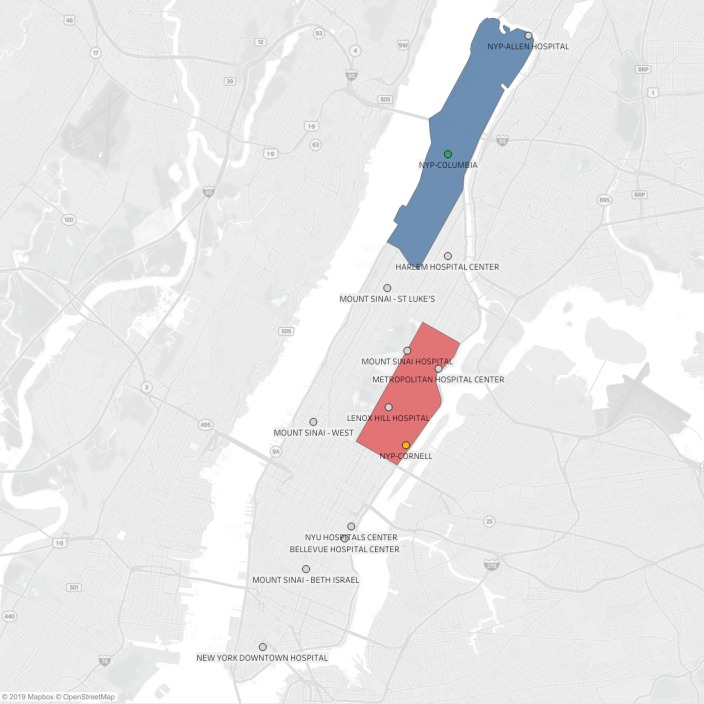
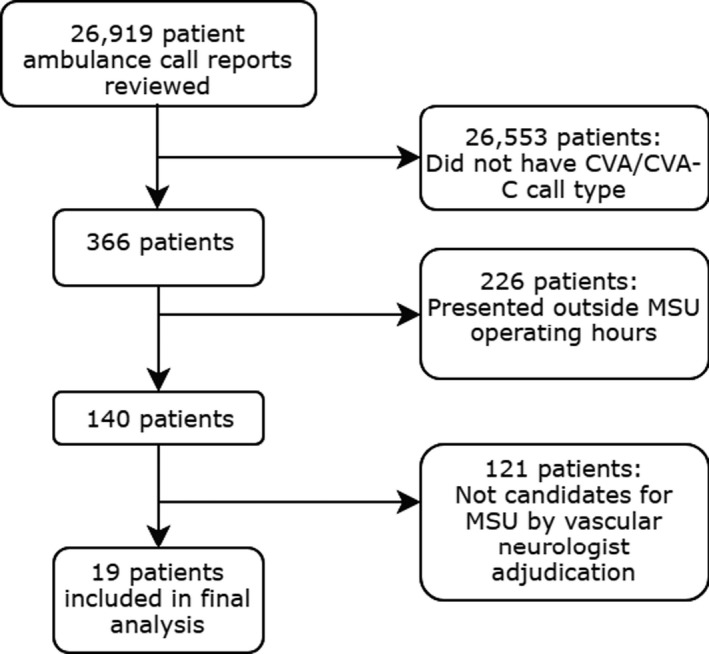
Background Mobile stroke units (MSUs) reduce time to intravenous thrombolysis in acute ischemic stroke. Whether this advantage exists in densely populated urban areas with many proximate hospitals is unclear. Methods and Results We evaluated patients from the METRONOME (Metropolitan New York Mobile Stroke) registry with suspected acute ischemic stroke who were transported by a bi-institutional MSU operating in Manhattan, New York, from October 2016 to September 2017. The comparison group included patients transported to our hospitals via conventional ambulance for acute ischemic stroke during the same hours of MSU operation (Monday to Friday, 9 am to 5 pm). Our exposure was MSU care, and our primary outcome was dispatch-to-thrombolysis time. We estimated mean differences in the primary outcome between both groups, adjusting for clinical, demographic, and geographic factors, including numbers of nearby designated stroke centers and population density. We identified 66 patients treated or transported by MSU and 19 patients transported by conventional ambulance. Patients receiving MSU care had significantly shorter dispatch-to-thrombolysis time than patients receiving conventional care (mean: 61.2 versus 91.6 minutes; P=0.001). Compared with patients receiving conventional care, patients receiving MSU care were significantly more likely to be picked up closer to a higher mean number of designated stroke centers in a 2.0-mile radius (4.8 versus 2.7, P=0.002). In multivariable analysis, MSU care was associated with a mean decrease in dispatch-to-thrombolysis time of 29.7 minutes (95% CI, 6.9-52.5) compared with conventional care. Conclusions In a densely populated urban area with a high number of intermediary stroke centers, MSU care was associated with substantially quicker time to thrombolysis compared with conventional ambulance care.
Keywords: acute ischemic stroke; geocoding; mobile stroke unit; prehospital stroke care; tissue plasminogen activator.
Figures
References
-
- Walter S, Kostopoulos P, Haass A, Keller I, Lesmeister M, Schlechtriemen T, Roth C, Papanagiotou P, Grunwald I, Schumacher H, Helwig S, Viera J, Körner H, Alexandrou M, Yilmaz U, Ziegler K, Schmidt K, Dabew R, Kubulus D, Liu Y, Volk T, Kronfeld K, Ruckes C, Bertsch T, Reith W, Fassbender K. Diagnosis and treatment of patients with stroke in a mobile stroke unit versus in hospital: a randomised controlled trial. Lancet Neurol. 2012;11:397–404. - PubMed
-
- Ebinger M, Winter B, Wendt M, Weber JE, Waldschmidt C, Rozanski M, Kunz A, Koch P, Kellner PA, Gierhake D, Villringer K, Fiebach JB, Grittner U, Hartmann A, Mackert BM, Endres M, Audebert HJ; STEMO Consortium . Effect of the use of ambulance‐based thrombolysis on time to thrombolysis in acute ischemic stroke: a randomized clinical trial. JAMA. 2014;311:1622–1631. - PubMed
-
- Itrat A, Taqui A, Cerejo R, Briggs F, Cho SM, Organek N, Reimer AP, Winners S, Rasmussen P, Hussain MS, Uchino K; Cleveland Pre‐Hospital Acute Stroke Treatment Group . Telemedicine in prehospital stroke evaluation and thrombolysis: taking stroke treatment to the doorstep. JAMA Neurol. 2016;73:162–168. - PubMed
-
- Taqui A, Cerejo R, Itrat A, Briggs FB, Reimer AP, Winners S, Organek N, Buletko AB, Sheikhi L, Cho SM, Buttrick M, Donohue MM, Khawaja Z, Wisco D, Frontera JA, Russman AN, Hustey FM, Kralovic DM, Rasmussen P, Uchino K, Hussain MS. Reduction in time to treatment in prehospital telemedicine evaluation and thrombolysis. Neurology. 2017;88:1305–1312. - PubMed
-
- Bowry R, Parker S, Rajan SS, Yamal JM, Wu TC, Richardson L, Noser E, Persse D, Jackson K, Grotta JC. Benefits of stroke treatment using a mobile stroke unit compared with standard management: the BEST‐MSU study run‐in phase. Stroke. 2015;46:3370–3374. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
