

Mean arterial blood pressure: potential predictive tool for preeclampsia in a cohort of healthy nulliparous pregnant women
- PMID: 31795971
- PMCID: PMC6892235
- DOI: 10.1186/s12884-019-2580-4
Mean arterial blood pressure: potential predictive tool for preeclampsia in a cohort of healthy nulliparous pregnant women
Abstract
Background: Prediction of preeclampsia is a challenge to overcome. The vast majority of prospective studies in large general obstetric populations have failed in the purpose of obtain a useful and effective model of prediction, sometimes based on complex tools unavaible in areas where the incidence of preeclampsia is the highest. The goal of this study was to assess mean arterial blood pressure (MAP) levels at 19-21, 27-29 and 37-39 weeks of gestation and performance of screening by MAP for the prediction of preeclampsia in a Brazilian cohort of healthy nulliparous pregnant women.
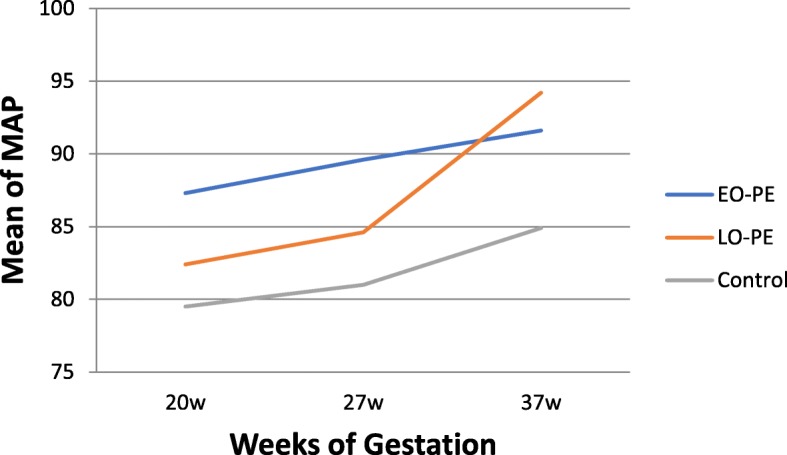
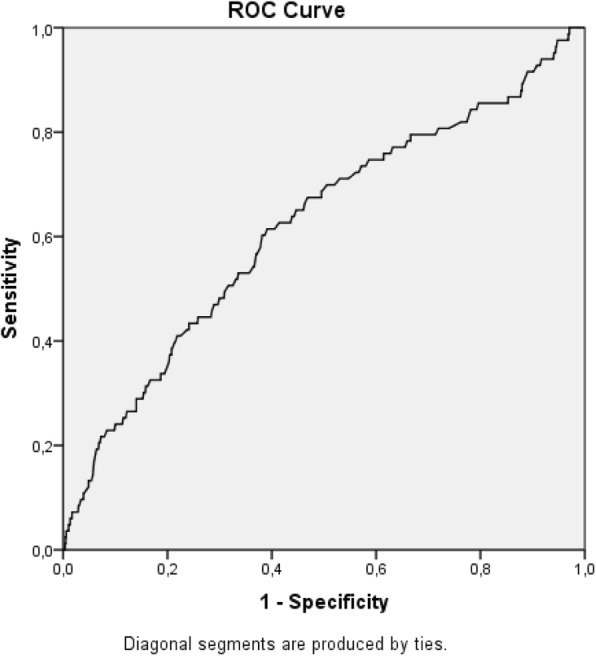
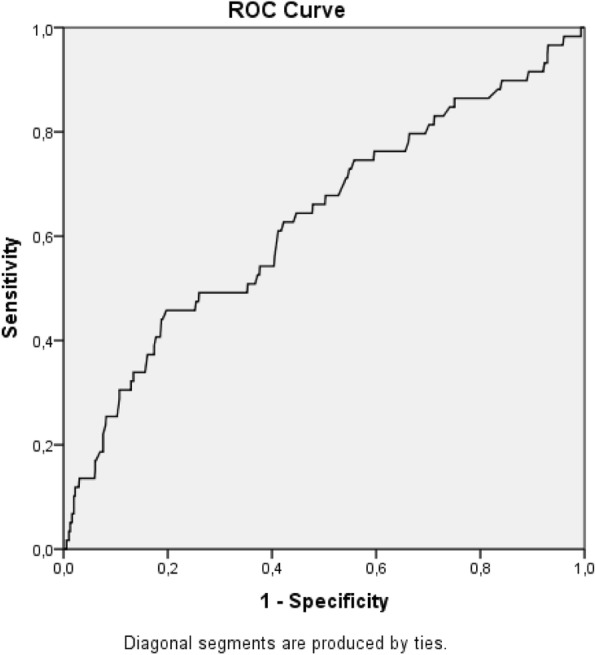
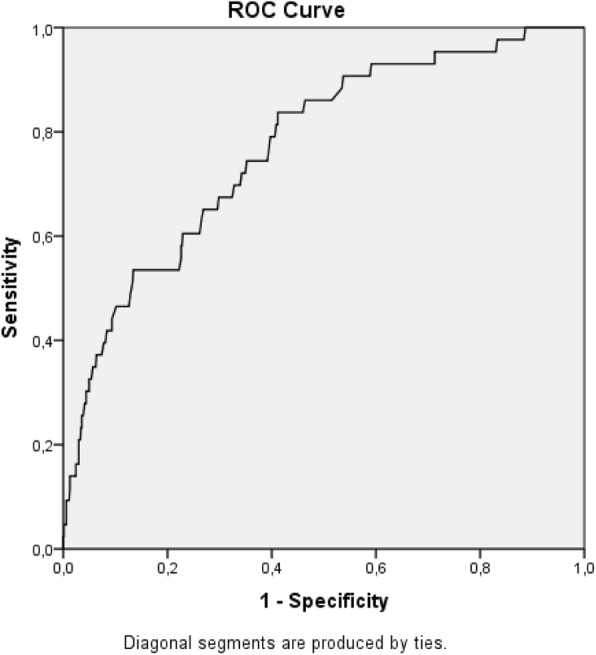
Methods: This was a cohort approach to a secondary analysis of the Preterm SAMBA study. Mean arterial blood pressure was evaluated at three different time periods during pregnancy. Groups with early-onset preeclampsia, late-onset preeclampsia and normotension were compared. Increments in mean arterial blood pressure between 20 and 27 weeks and 20 and 37 weeks of gestation were also calculated for the three groups studied. The accuracy of mean arterial blood pressure in the prediction of preeclampsia was determined by ROC curves.
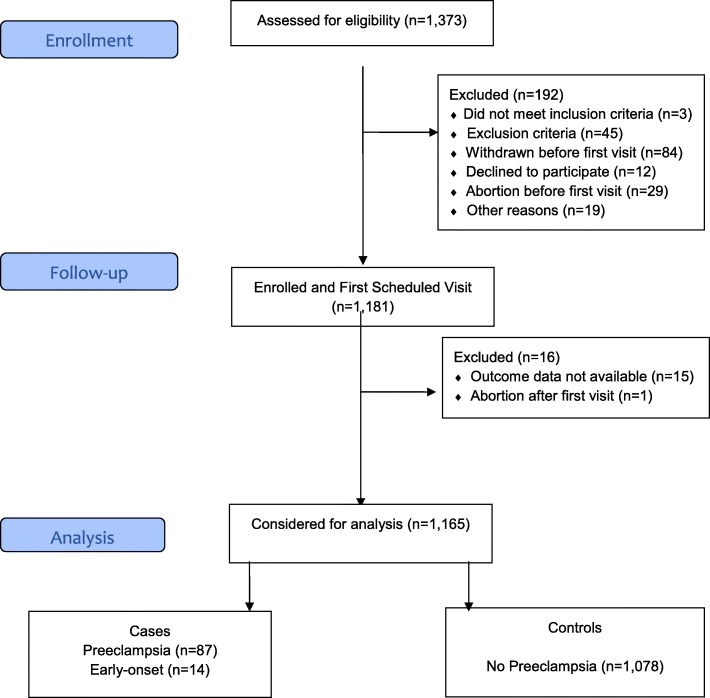
Results: Of the 1373 participants enrolled, complete data were available for 1165. The incidence of preeclampsia was 7.5%. Women with early-onset preeclampsia had higher mean arterial blood pressure levels at 20 weeks of gestation, compared to the normotensive group. Women with late-onset preeclampsia had higher mean arterial blood pressure levels at 37 weeks of gestation, than the normotensive groups and higher increases in this marker between 20 and 37 weeks of gestation. Based on ROC curves, the predictive performance of mean arterial blood pressure was higher at 37 weeks of gestation, with an area under the curve of 0.771.
Conclusion: As an isolated marker for the prediction of preeclampsia, the performance of mean arterial blood pressure was low in a healthy nulliparous pregnant women group. Considering that early-onset preeclampsia cases had higher mean arterial blood pressure levels at 20 weeks of gestation, future studies with larger cohorts that combine multiple markers are needed for the development of a preeclampsia prediction model.
Keywords: Blood pressure; Hypertension; Preeclampsia; Prenatal screening; Second trimester; Third trimester.
Conflict of interest statement
Maria L Costa, one of the co-authors is Associate Editor of the BMC Pregnancy and Childbirth. The other authors declare that they have no competing interests.
Figures
References
-
- Poon LC, Nicolaides KH. First-trimester maternal factors and biomarker screening for preeclampsia. Prenat Diagn. 2014;34(7):618–627. - PubMed
-
- O'Gorman N, Wright D, Poon LC, Rolnik DL, Syngelaki A, de Alvarado M, et al. Multicenter screening for pre-eclampsia by maternal factors and biomarkers at 11-13 weeks' gestation: comparison with NICE guidelines and ACOG recommendations. Ultrasound Obstet Gynecol. 2017;49(6):756–760. doi: 10.1002/uog.17455. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
