

Mortality risk and causes of death in patients with non-cystic fibrosis bronchiectasis
- PMID: 31796019
- PMCID: PMC6889428
- DOI: 10.1186/s12931-019-1243-3
Mortality risk and causes of death in patients with non-cystic fibrosis bronchiectasis
Abstract
Background: All-cause mortality risk and causes of death in bronchiectasis patients have not been fully investigated. The aim of this study was to compare the mortality risk and causes of death between individuals with bronchiectasis and those without bronchiectasis.
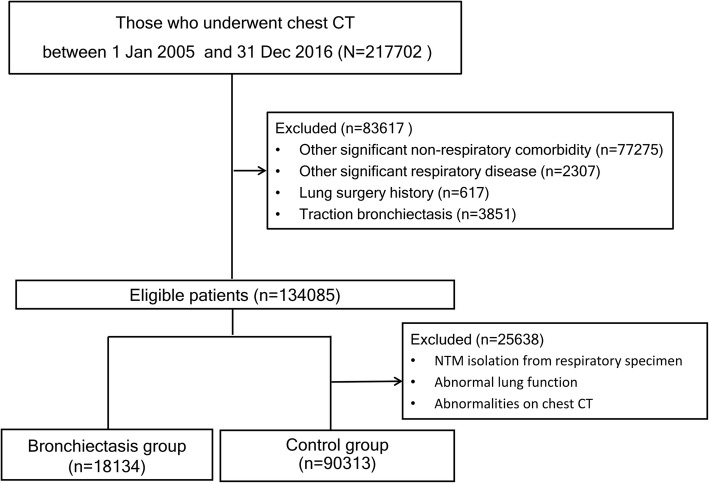
Methods: Patients with or without bronchiectasis determined based on chest computed tomography (CT) at one centre between 2005 and 2016 were enrolled. Among the patients without bronchiectasis, a control group was selected after applying additional exclusion criteria. We compared the mortality risk and causes of death between the bronchiectasis and control groups without lung disease. Subgroup analyses were also performed according to identification of Pseudomonas or non-tuberculous mycobacteria, airflow limitation, and smoking status.
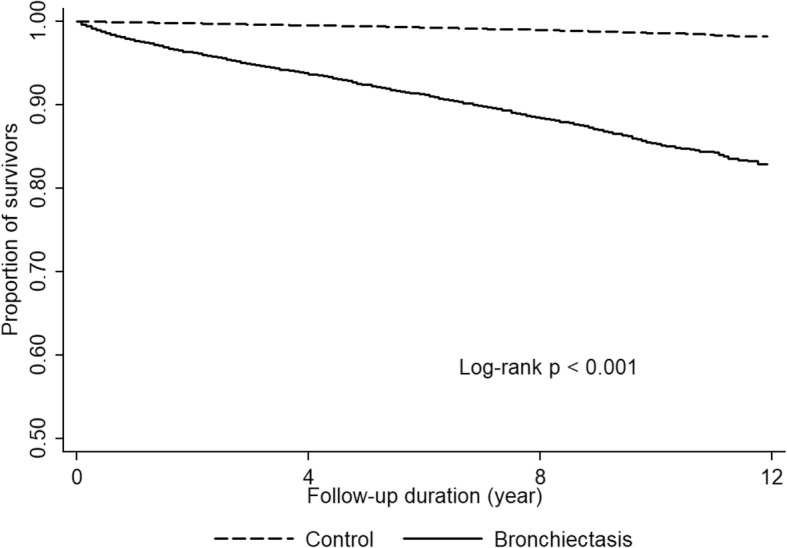
Results: Of the total 217,702 patients who underwent chest CT, 18,134 bronchiectasis patients and 90,313 non-bronchiectasis patients were included. The all-cause mortality rate in the bronchiectasis group was 1608.8 per 100,000 person-years (95% confidence interval (CI), 1531.5-1690.0), which was higher than that in the control group (133.5 per 100,000 person-years; 95% CI, 124.1-143.8; P < 0.001). The bronchiectasis group had higher all-cause (adjusted hazard ratio (aHR), 1.26; 95% CI, 1.09-1.47), respiratory (aHR, 3.49; 95% CI, 2.21-5.51), and lung cancer-related (aHR, 3.48; 95% CI, 2.33-5.22) mortality risks than the control group. In subgroup analysis, patients with airflow limitation and ever smokers showed higher all-cause mortality risk among bronchiectasis patients. Therefore, we observed significant interrelation between bronchiectasis and smoking, concerning the risks of all-cause mortality (P for multiplicative interaction, 0.030, RERI, 0.432; 95% CI, 0.097-0.769) and lung cancer-related mortality (RERI, 8.68; 95% CI, 1.631-15.736).
Conclusion: Individuals with bronchiectasis had a higher risk of all-cause, respiratory, and lung cancer-related mortality compared to control group. The risk of all-cause mortality was more prominent in those with airflow limitation and in ever smokers.
Keywords: Bronchiectasis; Cause of death; Mortality.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Weycker D, Edelsberg J, Oster G, Tino G. Prevalence and economic burden of bronchiectasis. Clin Pulm Med. 2005;12(4):205–209. doi: 10.1097/01.cpm.0000171422.98696.ed. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
