

Endoscopic dacryocystorhinostomy to treat congenital nasolacrimal canal dysplasia: a retrospective analysis in 40 children
- PMID: 31796021
- PMCID: PMC6889731
- DOI: 10.1186/s12886-019-1256-1
Endoscopic dacryocystorhinostomy to treat congenital nasolacrimal canal dysplasia: a retrospective analysis in 40 children
Abstract
Background: To investigate the therapeutic effectiveness and safety of endoscopic dacryocystorhinostomy (EN-DCR) to treat congenital nasolacrimal canal dysplasia (CNCD).
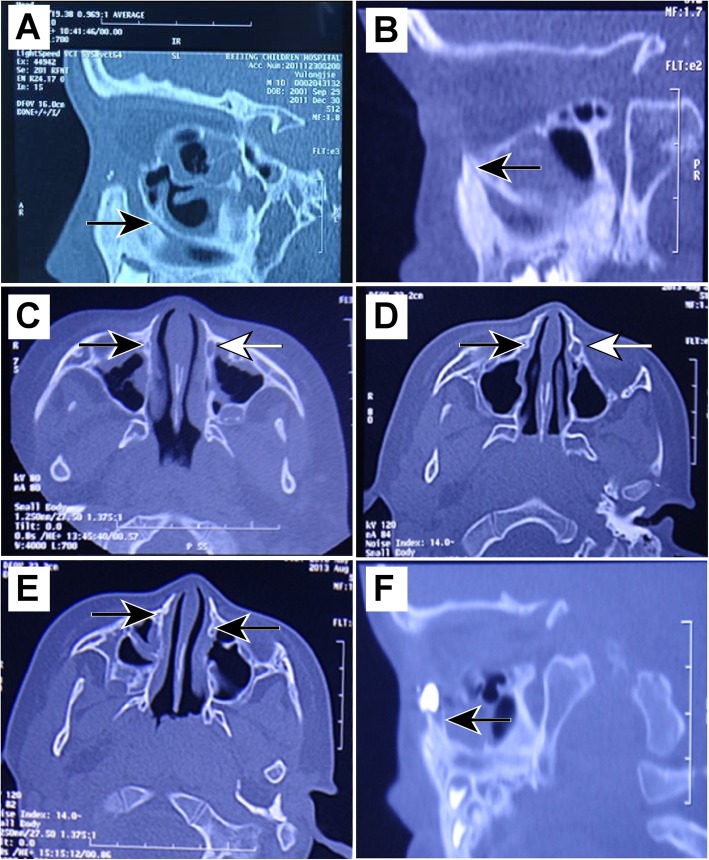
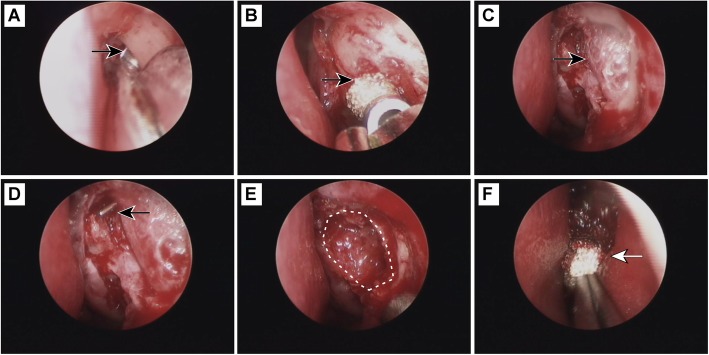
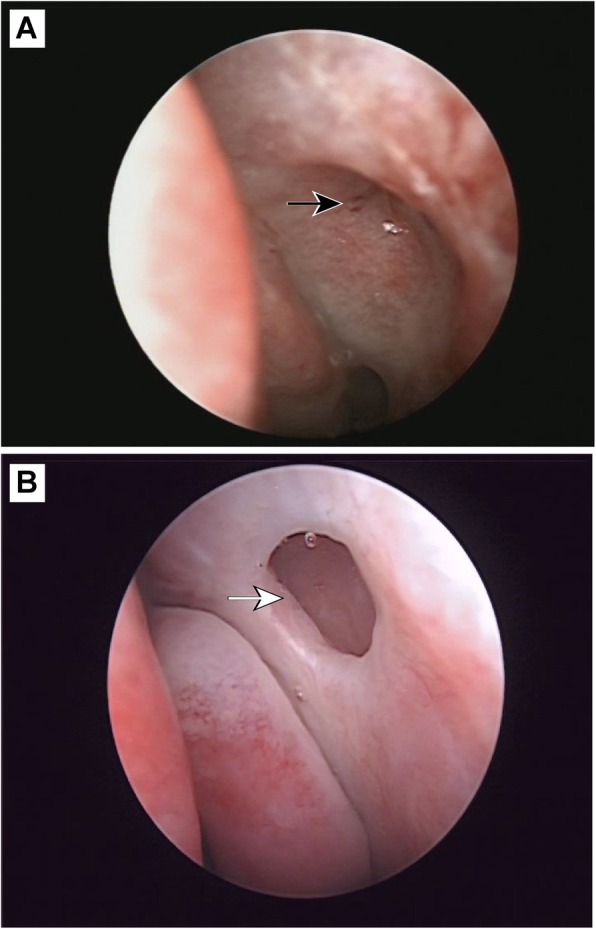
Methods: Forty children (50 eyes) with congenital nasolacrimal duct obstruction (CNLDO) and lacrimal bony dysplasia, including 8 children with bony atresia (10 eyes) and 32 with bony stenosis (40 eyes), were recruited in this retrospective study. Standardized EN-DCR was performed in all cases. The postoperative observations included relief of symptoms, fluorescein dye disappearance test (FDDT), syringing of lacrimal passages and anastomotic patency under nasal endoscopy. Patients were followed up for 8-18 months.
Results: Standardized EN-DCR surgery had a success (cure and improvement) rate of 100%, including a cure rate of 82% and an improvement rate of 18%. The cure rate among 40 cases of bony nasolacrimal duct stenosis was 82.5%, while that of 10 cases of bony nasolacrimal duct atresia was 80%. Statistical analysis showed that nether the receipt of other treatments before surgery nor the type of bony nasolacrimal duct dysplasia affected the cure rate. No significant complications were observed during postoperative follow-up except for four cases (4 eyes) that suffered middle turbinate and nasal mucosal adhesion and two cases with sinusitis.
Conclusions: CNCD is a type of CNLDO that does not respond to conservative and conventional treatment. EN-DCR represents a safe and effective treatment for children with CNCD. In addition, the combination of EN-DCR with lacrimal CT scanning provides advantages over traditional lacrimal surgery in that it has a high success rate with a low incidence of complications.
Keywords: Children; Congenital nasolacrimal duct obstruction (CNLDO); Endoscopic dacryocystorhinostomy (EN-DCR); Nasal endoscopy; Nasolacrimal canal dysplasia.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Yu G, Zhang CY, Cui YH, Fan YW, Cao WH, Lin Q, et al. Application value of computed tomography dacryocystography in children lacrimal diseases. Zhonghua Yan Ke Za Zhi. 2013;49:706–710. - PubMed
MeSH terms
Grants and funding
- No. 81570891/National Natural Science Foundation of China
- No. 7151003/Beijing Natural Science Foundation
- No. 2014-2-003/Advanced Health Care Professionals Development Project of Beijing Municipal Health Bureau
- DFL20150201/Beijing Municipal Administration of Hospitals' Ascent Plan
- 2016-1-2051/The Capital Health Research and Development of Special
- ZYLX201307/Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support
- Z181100001818003/Science & Technology Project of Beijing Municipal Science & Technology Commission
- Z151100001615052/Science & Technology Project of Beijing Municipal Science & Technology Commission
LinkOut - more resources
Full Text Sources
Research Materials
