

Worsening and newly diagnosed paraneoplastic syndromes following anti-PD-1 or anti-PD-L1 immunotherapies, a descriptive study
- PMID: 31796119
- PMCID: PMC6892018
- DOI: 10.1186/s40425-019-0821-8
Worsening and newly diagnosed paraneoplastic syndromes following anti-PD-1 or anti-PD-L1 immunotherapies, a descriptive study
Abstract
Background: Paraneoplastic syndromes (PNS) are autoimmune disorders specifically associated with cancer. There are few data on anti-PD-1 or anti-PD-L1 immunotherapy in patients with a PNS. Our objective was to describe the outcome for patients with a pre-existing or newly diagnosed PNS following the initiation of anti-PD-1 or anti-PD-L1 immunotherapy.
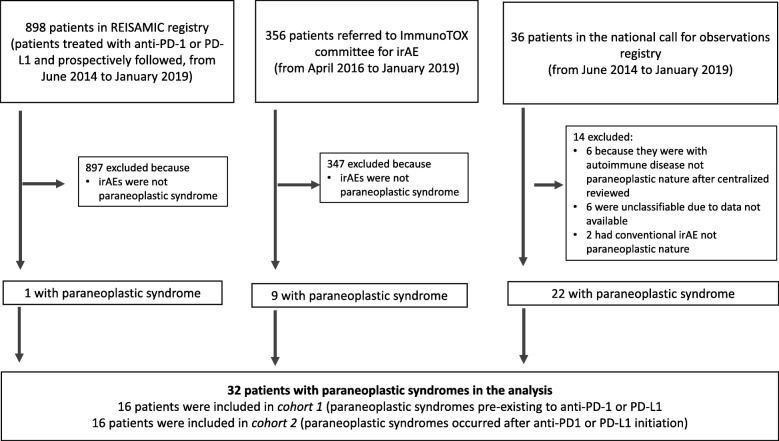
Methods: We included all adult patients (aged ≥18) treated with anti-PD-1 or anti-PD-L1 immunotherapy for a solid tumor, diagnosed with a PNS, and registered in French pharmacovigilance databases. Patients were allocated to cohorts 1 and 2 if the PNS had been diagnosed before vs. after the initiation of immunotherapy, respectively.
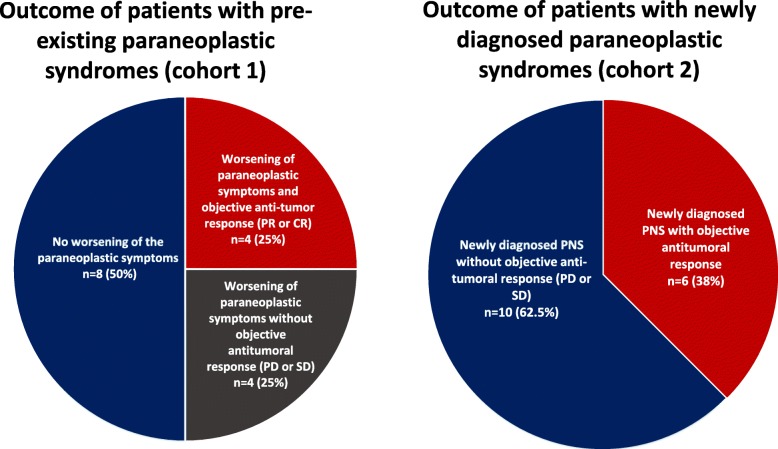
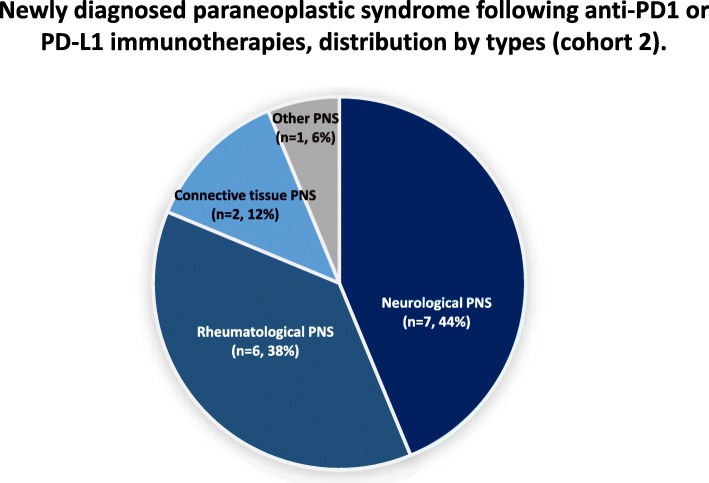
Findings: Of the 1304 adult patients screened between June 27th, 2014, and January 2nd, 2019, 32 (2.45%) had a PNS and were allocated to either cohort 1 (n = 16) or cohort 2 (n = 16). The median (range) age was 64 (45-88). The tumor types were non-small-cell lung cancer (n = 15, 47%), melanoma (n = 6, 19%), renal carcinoma (n = 3, 9%), and other malignancies (n = 8, 25%). Eleven (34%) patients presented with a neurologic PNS, nine (28%) had a rheumatologic PNS, eight (25%) had a connective tissue PNS, and four (13%) had other types of PNS. The highest severity grade for the PNS was 1-2 in 10 patients (31%) and ≥ 3 in 22 patients (69%). Four patients (13%) died as a result of the progression of a neurologic PNS (encephalitis in three cases, and Lambert-Eaton syndrome in one case). Following the initiation of immunotherapy, the PNS symptoms worsened in eight (50%) of the 16 patients in cohort 1.
Interpretation: Our results show that PNSs tend to be worsened or revealed by anti-PD-1 or anti-PD-L1 immunotherapy. Cases of paraneoplastic encephalitis are of notable concern, in view of their severity. When initiating immunotherapy, physicians should carefully monitor patients with a pre-existing PNS.
Conflict of interest statement
The authors have the following competing interests to disclose:
Dr. Jean-Marie Michot:
Principal/sub-Investigator of Clinical Trials for: Abbvie, Aduro, Agios, Amgen, Argen-x, Astex, AstraZeneca, Aveo pharmaceuticals, Bayer, Beigene, Blueprint, BMS, Boeringer Ingelheim, Celgene, Chugai, Clovis, Daiichi Sankyo, Debiopharm, Eisai, Eos, Exelixis, Forma, Gamamabs, Genentech, Gortec, GSK, H3 biomedecine, Incyte, Innate Pharma, Janssen, Kura Oncology, Kyowa, Lilly, Loxo, Lysarc, Lytix Biopharma, Medimmune, Menarini, Merus, MSD, Nanobiotix, Nektar Therapeutics, Novartis, Octimet, Oncoethix, Oncopeptides AB, Orion, Pfizer, Pharmamar, Pierre Fabre, Roche, Sanofi, Servier, Sierra Oncology, Taiho, Takeda, Tesaro, Xencor.
Personal fees (monies paid for services rendered, generally honoraria, royalties or fees for consulting, lectures, speakers bureaus, expert testimony, employment, ad-boards, etc.): Roche, Celgene, Bristol-Myers Squibb, AstraZeneca, Janssen.
Dr. Christophe Massard:
Principal/sub-Investigator of Clinical Trials for: Abbvie, Aduro, Agios, Amgen, Argen-x, Astex, AstraZeneca, Aveo pharmaceuticals, Bayer, Beigene, Blueprint, BMS, Boeringer Ingelheim, Celgene, Chugai, Clovis, Daiichi Sankyo, Debiopharm, Eisai, Eos, Exelixis, Forma, Gamamabs, Genentech, Gortec, GSK, H3 biomedecine, Incyte, Innate Pharma, Janssen, Kura Oncology, Kyowa, Lilly, Loxo, Lysarc, Lytix Biopharma, Medimmune, Menarini, Merus, MSD, Nanobiotix, Nektar Therapeutics, Novartis, Octimet, Oncoethix, Oncopeptides AB, Orion, Pfizer, Pharmamar, Pierre Fabre, Roche, Sanofi, Servier, Sierra Oncology, Taiho, Takeda, Tesaro, Xencor.
Personal fees (Monies paid for services rendered, generally honoraria, royalties or fees for consulting, lectures, speakers bureaus, expert testimony, employment, ad-boards, etc.): Medimmune, Lilly, Bristol-Myers Squibb.
Dr. Aurélien Marabelle:
Principal/sub-Investigator of Clinical Trials for: Abbvie, Aduro, Agios, Amgen, Argen-x, Astex, AstraZeneca, Aveo pharmaceuticals, Bayer, Beigene, Blueprint, BMS, Boeringer Ingelheim, Celgene, Chugai, Clovis, Daiichi Sankyo, Debiopharm, Eisai, Eos, Exelixis, Forma, Gamamabs, Genentech, Gortec, GSK, H3 biomedecine, Incyte, Innate Pharma, Janssen, Kura Oncology, Kyowa, Lilly, Loxo, Lysarc, Lytix Biopharma, Medimmune, Menarini, Merus, MSD, Nanobiotix, Nektar Therapeutics, Novartis, Octimet, Oncoethix, Oncopeptides AB, Orion, Pfizer, Pharmamar, Pierre Fabre, Roche, Sanofi, Servier, Sierra Oncology, Taiho, Takeda, Tesaro, Xencor.
Personal fees (Monies paid for services rendered, generally honoraria, royalties or fees for consulting, lectures, speakers bureaus, expert testimony, employment, ad-boards, etc.): AstraZeneca, Medimmune, MSD, Tesaro.
Professor Olivier Lambotte:
Reports personal fees from BMS, MSD, AstraZeneca, and Genzyme and non-financial support from LFB, BMS, and CSL Behring.
All other authors declare no competing interests.
Figures
References
-
- Menzies AM, Johnson DB, Ramanujam S, et al. Anti-PD-1 therapy in patients with advanced melanoma and preexisting autoimmune disorders or major toxicity with ipilimumab. Ann Oncol Off J Eur Soc Med Oncol. 2017;28:368–376. - PubMed
-
- Le Burel S, Champiat S, Mateus C, et al. Prevalence of immune-related systemic adverse events in patients treated with anti-Programmed cell Death 1/anti-Programmed cell Death-Ligand 1 agents: A single-centre pharmacovigilance database analysis. Eur J Cancer Oxf Engl. 2017;82:34–44. doi: 10.1016/j.ejca.2017.05.032. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials