

Temporal trends in the use of targeted temperature management after cardiac arrest and association with outcome: insights from the Paris Sudden Death Expertise Centre
- PMID: 31796127
- PMCID: PMC6892202
- DOI: 10.1186/s13054-019-2677-1
Temporal trends in the use of targeted temperature management after cardiac arrest and association with outcome: insights from the Paris Sudden Death Expertise Centre
Abstract
Purpose: Recent doubts regarding the efficacy may have resulted in a loss of interest for targeted temperature management (TTM) in comatose cardiac arrest (CA) patients, with uncertain consequences on outcome. We aimed to identify a change in TTM use and to assess the relationship between this change and neurological outcome.
Methods: We used Utstein data prospectively collected in the Sudden Death Expertise Center (SDEC) registry (capturing CA data from all secondary and tertiary hospitals located in the Great Paris area, France) between May 2011 and December 2017. All cases of non-traumatic OHCA patients with stable return of spontaneous circulation (ROSC) were included. After adjustment for potential confounders, we assessed the relationship between changes over time in the use of TTM and neurological recovery at discharge using the Cerebral Performance Categories (CPC) scale.
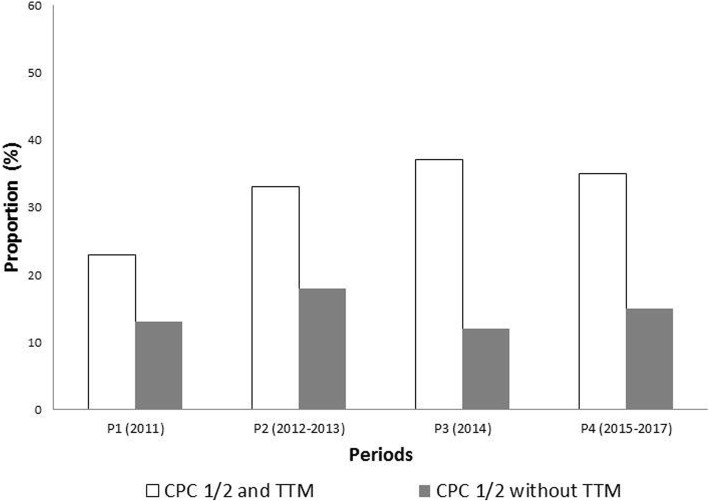
Results: Between May 2011 and December 2017, 3925 patients were retained in the analysis, of whom 1847 (47%) received TTM. The rate of good neurological outcome at discharge (CPC 1 or 2) was higher in TTM patients as compared with no TTM (33% vs 15%, P < 0.001). Gender, age, and location of CA did not change over the years. Bystander CPR increased from 55% in 2011 to 73% in 2017 (P < 0.001) and patients with a no-flow time longer than 3 min decreased from 53 to 38% (P < 0.001). The use of TTM decreased from 55% in 2011 to 37% in 2017 (P < 0.001). Meanwhile, the rate of patients with good neurological recovery remained stable (19 to 23%, P = 0.76). After adjustment, year of CA occurrence was not associated with outcome.
Conclusions: We report a progressive decrease in the use of TTM in post-cardiac arrest patients over the recent years. During this period, neurological outcome remained stable, despite an increase in bystander-initiated resuscitation and a decrease in "no flow" duration.
Keywords: Cardiac arrest; Induced hypothermia; Neurological outcome; Targeted temperature management.
Conflict of interest statement
AC received fees for lectures from C.R. Bard (Murray Hill, NJ, USA). The other authors declare that they have no competing interests.
Figures


References
-
- Kragholm Kristian, Wissenberg Mads, Mortensen Rikke N., Hansen Steen M., Malta Hansen Carolina, Thorsteinsson Kristinn, Rajan Shahzleen, Lippert Freddy, Folke Fredrik, Gislason Gunnar, Køber Lars, Fonager Kirsten, Jensen Svend E., Gerds Thomas A., Torp-Pedersen Christian, Rasmussen Bodil S. Bystander Efforts and 1-Year Outcomes in Out-of-Hospital Cardiac Arrest. New England Journal of Medicine. 2017;376(18):1737–1747. doi: 10.1056/NEJMoa1601891. - DOI - PubMed
-
- Dumas F, Grimaldi D, Zuber B, Fichet J, Charpentier J, Pene F, Vivien B, Varenne O, Carli P, Jouven X, et al. Is hypothermia after cardiac arrest effective in both shockable and nonshockable patients? Insights from a large registry. Circulation. 2011;123(8):877–886. doi: 10.1161/CIRCULATIONAHA.110.987347. - DOI - PubMed
-
- Salter R, Bailey M, Bellomo R, Eastwood G, Goodwin A, Nielsen N, Pilcher D, Nichol A, Saxena M, Shehabi Y, et al. Changes in temperature management of cardiac arrest patients following publication of the target temperature management trial. Crit Care Med. 2018;46(11):1722–1730. doi: 10.1097/CCM.0000000000003339. - DOI - PubMed
