

Adhesion reformation and the limited translational value of experiments with adhesion barriers: A systematic review and meta-analysis of animal models
- PMID: 31796777
- PMCID: PMC6890766
- DOI: 10.1038/s41598-019-52457-2
Adhesion reformation and the limited translational value of experiments with adhesion barriers: A systematic review and meta-analysis of animal models
Abstract
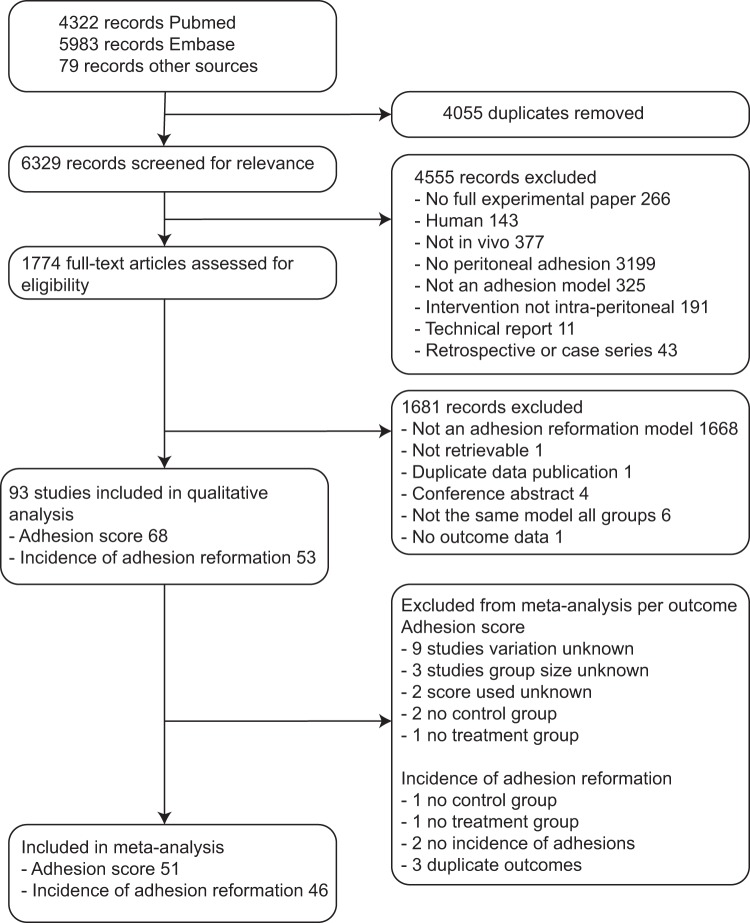
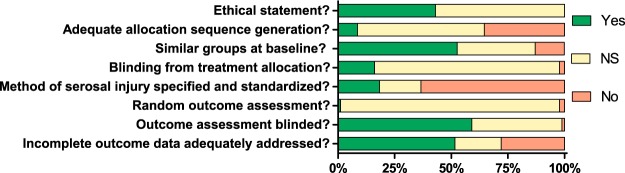
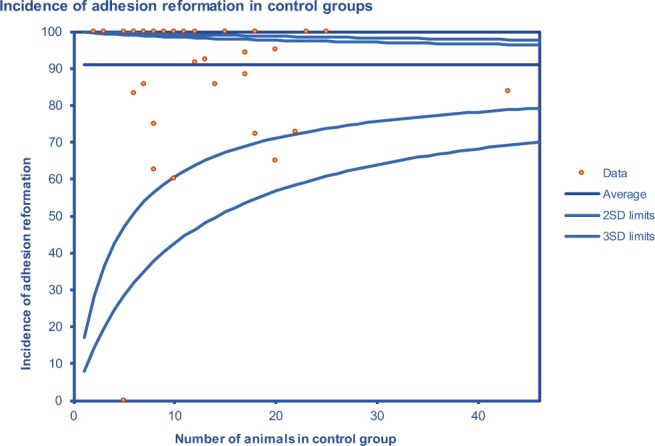
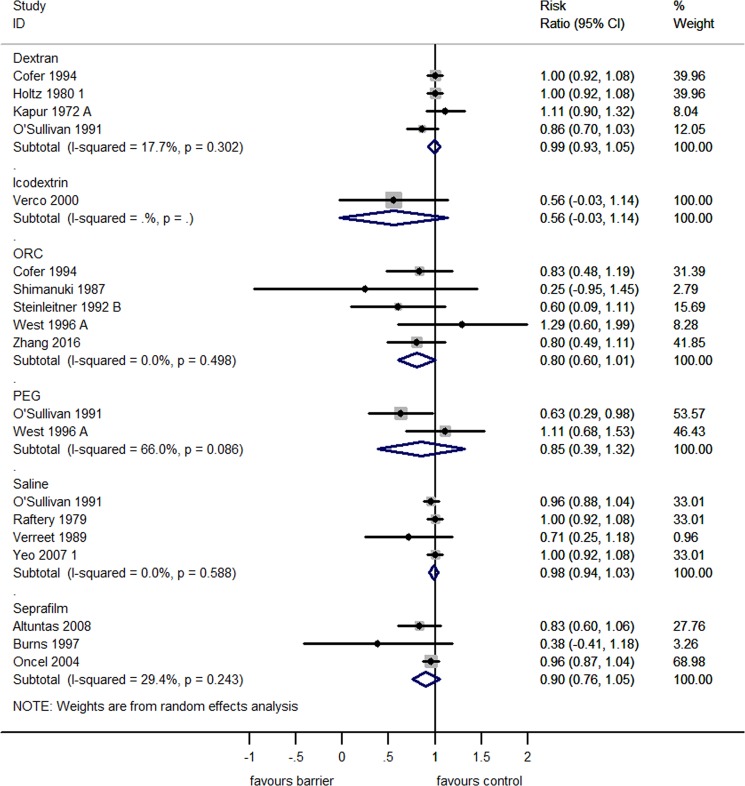
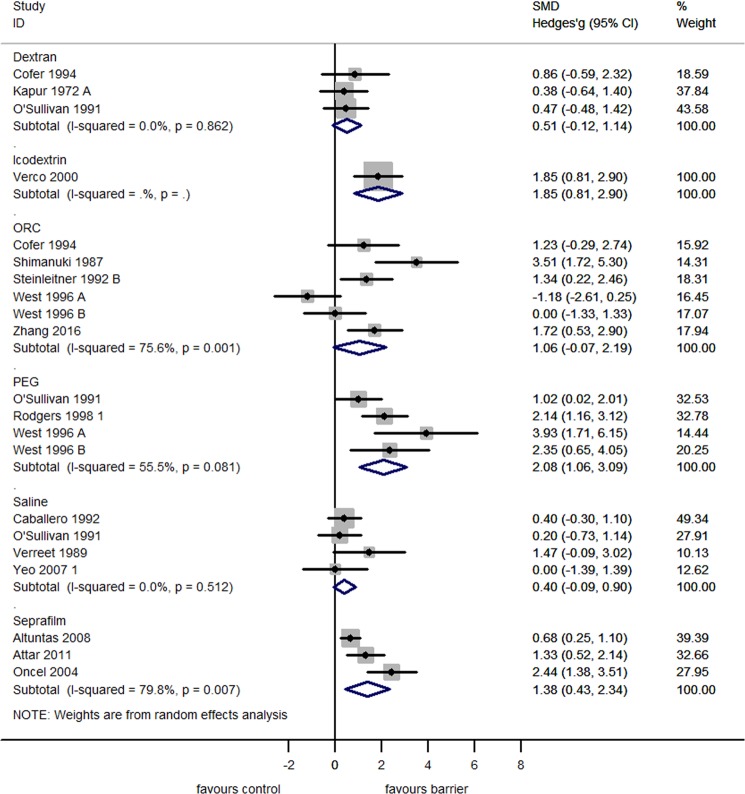
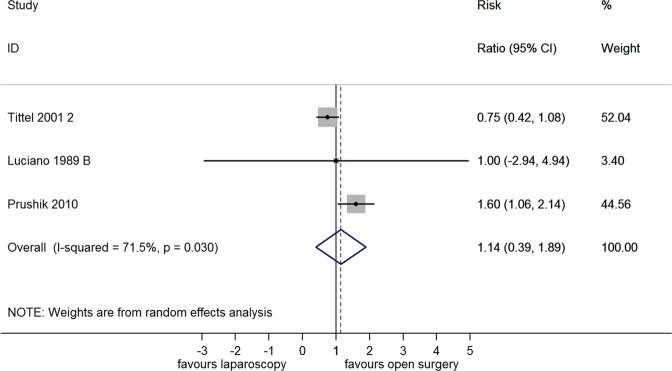
Today, 40-66% of elective procedures in general surgery are reoperations. During reoperations, the need for adhesiolysis results in increased operative time and a more complicated convalescence. In pre-clinical evaluation, adhesion barriers are tested for their efficacy in preventing 'de novo' adhesion formation, However, it is unknown to which extent barriers are tested for prevention of adhesion reformation. The aim of this systematic review and meta-analysis is to assess the efficacy of commercially available adhesion barriers and laparoscopic adhesiolysis in preventing adhesion reformation in animal models. Pubmed and EMBASE were searched for studies which assessed peritoneal adhesion reformation after a standardized peritoneal injury (in the absence of an intra-peritoneal mesh), and reported the incidence of adhesions, or an adhesion score as outcome. Ninety-three studies were included. No study met the criteria for low risk of bias. None of the commercially available adhesion barriers significantly reduced the incidence of adhesion reformation. Three commercially available adhesion barriers reduced the adhesion score of reformed adhesions, namely Seprafilm (SMD 1.38[95% CI]; p < 0.01), PEG (SMD 2.08[95% CI]; p < 0.01) and Icodextrin (SMD 1.85[95% CI]; p < 0.01). There was no difference between laparoscopic or open adhesiolysis with regard to the incidence of adhesion reformation (RR 1.14[95% CI]; p ≥ 0.05) or the adhesion score (SMD 0.92[95% CI]; p ≥ 0.05). Neither currently commercially available adhesion barriers, nor laparoscopic adhesiolysis without using an adhesion barrier, reduces the incidence of adhesion reformation in animal models. The methodological quality of animal studies is poor.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Peritoneal adhesions after laparoscopic gastrointestinal surgery.World J Gastroenterol. 2014 May 7;20(17):4917-25. doi: 10.3748/wjg.v20.i17.4917. World J Gastroenterol. 2014. PMID: 24803803 Free PMC article. Review.
-
Efficacy of melatonin and hyaluronate/carboxymethylcellulose membrane in preventing adhesion reformation following adhesiolysis in a rat uterine model.J Obstet Gynaecol Res. 2011 Feb;37(2):125-31. doi: 10.1111/j.1447-0756.2010.01329.x. Epub 2010 Dec 16. J Obstet Gynaecol Res. 2011. PMID: 21159036 Clinical Trial.
-
Ultrapure alginate gel reduces adhesion reformation after adhesiolysis.Int J Colorectal Dis. 2014 Nov;29(11):1411-6. doi: 10.1007/s00384-014-2009-5. Epub 2014 Sep 13. Int J Colorectal Dis. 2014. PMID: 25213585
-
A randomized, controlled pilot study of the safety and efficacy of 4% icodextrin solution in the reduction of adhesions following laparoscopic gynaecological surgery.Hum Reprod. 2002 Apr;17(4):1031-8. doi: 10.1093/humrep/17.4.1031. Hum Reprod. 2002. PMID: 11925401 Clinical Trial.
-
Research progress on animal models of peritoneal adhesion.Surgery. 2025 Feb;178:108929. doi: 10.1016/j.surg.2024.10.020. Epub 2024 Nov 29. Surgery. 2025. PMID: 39613659 Review.
Cited by
-
Effects of antenatal corticosteroid therapy in animal models of fetal growth restriction: a systematic review and meta-analysis.BMC Pregnancy Childbirth. 2025 Mar 13;25(1):281. doi: 10.1186/s12884-025-07359-9. BMC Pregnancy Childbirth. 2025. PMID: 40082797 Free PMC article.
-
Prevention of post-operative adhesions: Model development and pilot outcomes of human placental stem cell-based interventions.Transfusion. 2024 Jun;64(6):1059-1067. doi: 10.1111/trf.17859. Epub 2024 May 1. Transfusion. 2024. PMID: 38693056 Free PMC article.
-
Prevention of Post-Operative Adhesions: A Comprehensive Review of Present and Emerging Strategies.Biomolecules. 2021 Jul 14;11(7):1027. doi: 10.3390/biom11071027. Biomolecules. 2021. PMID: 34356652 Free PMC article. Review.
-
Integrating Genomics and Molecular Biology in Understanding Peritoneal Adhesion.Curr Issues Mol Biol. 2025 Jun 19;47(6):475. doi: 10.3390/cimb47060475. Curr Issues Mol Biol. 2025. PMID: 40699873 Free PMC article. Review.
-
Adhesive small bowel obstruction - an update.Acute Med Surg. 2020 Nov 4;7(1):e587. doi: 10.1002/ams2.587. eCollection 2020 Jan-Dec. Acute Med Surg. 2020. PMID: 33173587 Free PMC article. Review.
References
-
- Colon Cancer Laparoscopic or Open Resection Study, G. et al., Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. The Lancet Oncology. 10(1) p, 44–52 (2009). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
