

What Works and What Doesn't Work? A Systematic Review of Digital Mental Health Interventions for Depression and Anxiety in Young People
- PMID: 31798468
- PMCID: PMC6865844
- DOI: 10.3389/fpsyt.2019.00759
What Works and What Doesn't Work? A Systematic Review of Digital Mental Health Interventions for Depression and Anxiety in Young People
Abstract
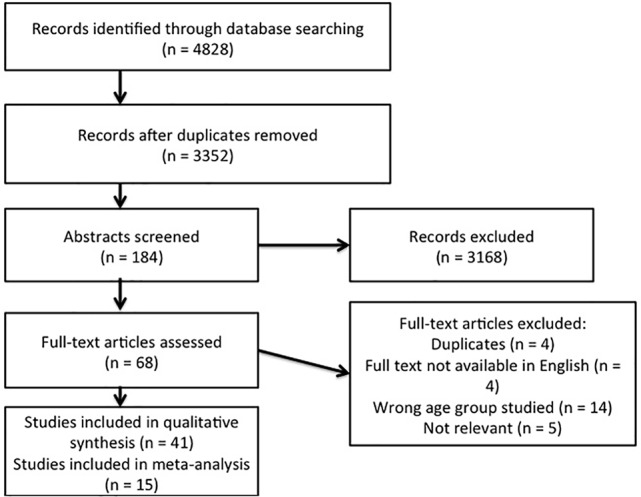
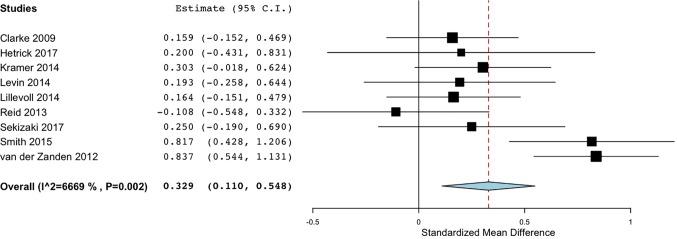
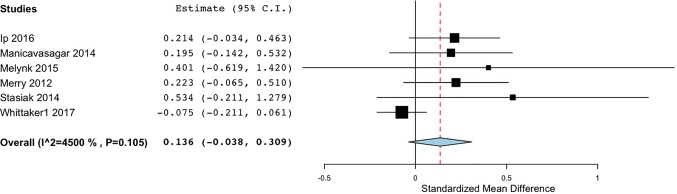
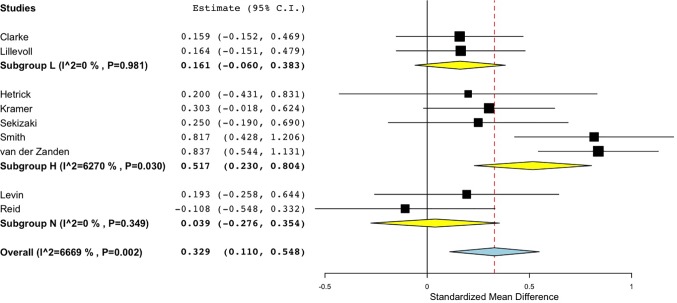
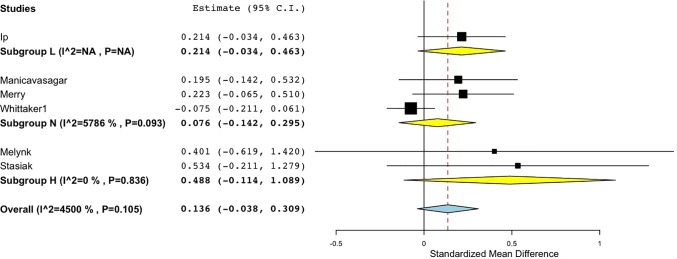
Background: A major challenge in providing mental health interventions for young people is making such interventions accessible and appealing to those most in need. Online and app-based forms of therapy for mental health are burgeoning. It is therefore crucial to identify features that are most effective and engaging for young users. Objectives: This study reports a systematic review and meta-analysis of digital mental health interventions and their effectiveness in addressing anxiety and depression in young people to determine factors that relate to outcomes, adherence, and engagement with such interventions. Methods: A mixed methods approach was taken, including a meta-analysis of 9 randomized controlled trials that compared use of a digital intervention for depression in young people to a no-intervention control group, and 6 comparing the intervention to an active control condition. A thematic analysis and narrative synthesis of 41 studies was also performed. Results: The pooled effect size of digital mental health interventions on depression in comparison to a no-intervention control was small (Cohen's d = 0.33, 95% CI 0.11 to 0.55), while the pooled effect size of studies comparing an intervention group to an active control showed no significant differences (Cohen's d = 0.14, 95% CI -.04 to 0.31). Pooled effect sizes were higher when supervision was involved (studies with no-intervention controls: Cohen's d = 0.52, 95% CI 0.23 to 0.80; studies with active control: Cohen's d = 0.49, 95% CI -0.11, 1.01). Engagement and adherence rates were low. Qualitative analysis revealed that users liked interventions with a game-like feel and relatable, interactive content. Educational materials were perceived as boring, and users were put off by non-appealing interfaces and technical glitches. Conclusions: Digital interventions work better than no intervention to improve depression in young people when results of different studies are pooled together. However, these interventions may only be of clinical significance when use is highly supervised. Digital interventions do not work better than active alternatives regardless of the level of support. Future interventions need to move beyond the use of digital educational materials, considering other ways to attract and engage young people and to ensure relevance and appeal.
Keywords: adolescents; children; low mood; prevention; self-management; unguided self-help.
Copyright © 2019 Garrido, Millington, Cheers, Boydell, Schubert, Meade and Nguyen.
Figures
References
-
- Lawrence D, Johnson S, Hafekost J, Boterhoven De Hann K, Sawyer M, Ainley J, et al. The mental health of children and adolescents. Report on the second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Canberra: Department of Health; (2015).
-
- Merikangas KR, He J, Burstein M, Swanson SA, Avenevoli S, Cui L, et al. Lifetime prevalence of mental disorders in U. S. adolescents: results from the national comorbidity survey replication - adolescent supplement (NCS-A). J Am Acad Child AdolescPsychiatry (2010) 49(10):980–9. 10.1016/j.jaac.2010.05.017 - DOI - PMC - PubMed
-
- WHO Depression and other common mental disorders: Global health estimates (2017). Available from: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017....
-
- Davies S. Annual report of the chief medical officer 2013, public mental health priorities: Inesting in the evidence. London, UK: Department of Health; (2014).
Publication types
LinkOut - more resources
Full Text Sources
Medical