

Variation of Mass Effect After Using a Flow Diverter With Adjunctive Coil Embolization for Symptomatic Unruptured Large and Giant Intracranial Aneurysms
- PMID: 31798519
- PMCID: PMC6874129
- DOI: 10.3389/fneur.2019.01191
Variation of Mass Effect After Using a Flow Diverter With Adjunctive Coil Embolization for Symptomatic Unruptured Large and Giant Intracranial Aneurysms
Abstract
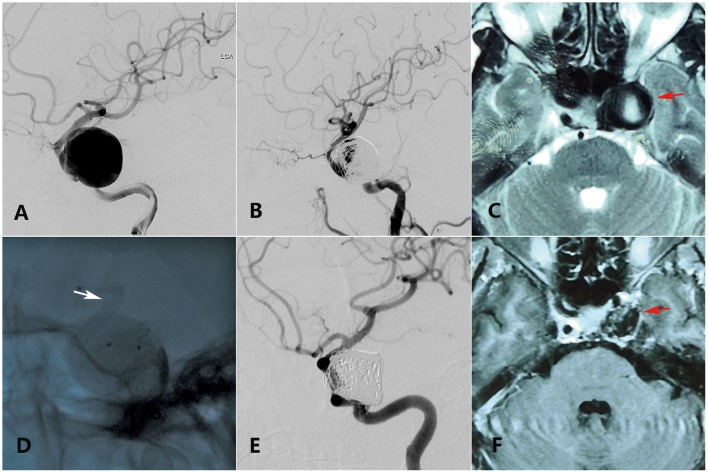
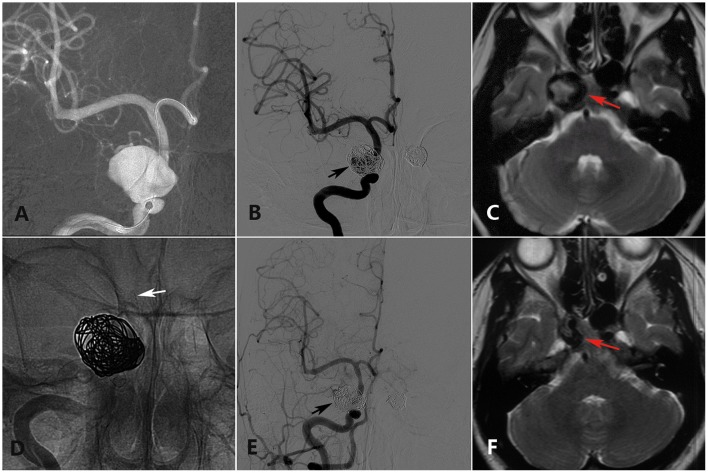
Background: Mass effect associated with large or giant aneurysms is an intractable problem for traditional endovascular treatments. Preventing recurrence of aneurysms requires dense coiling, which may aggravate the mass effect. However, the flow diverter (FD) is a new device that avoids the need for dense coiling. This study was performed to investigate whether use of FDs with adjunctive coil embolization can relieve the aneurysmal mass effect and to explore the factors that affect the variation of compressional symptoms. Methods: We retrospectively evaluated patients with compressional symptoms caused by unruptured aneurysms who underwent endovascular treatment with an FD with adjunctive coil embolization at our center from January 2015 to December 2017. Imaging follow-up included digital subtraction angiography (DSA) ranging from 11 to 14 months and magnetic resonance imaging (MRI) ranging from 24 to 30 months; the former was used to evaluate the intracavitary volume, and the latter was used to measure the variation of the mass effect. Follow-up physical examinations were performed to observe variations of symptoms. Results: In total, 22 patients with 22 aneurysms were treated by an FD combined with coil embolization. All 22 patients underwent the last clinical follow-up. Regarding compressional symptoms, 12 (54.54%) patients showed improvement, 6 (27.27%) were fully recovered, and 6 (27.27%) showed improvement but with incomplete cranial palsy. However, five (22.72%) patients showed no change, four (18.18%) showed worsening symptoms compared with their preoperative state, and one (4.55%) died of delayed rupture. Seventeen of the 22 patients underwent MRI. Of these 17 patients, the aneurysm shrank in 13 (76.47%) and no significant change occurred in 4 (23.53%). In the multivariate analysis, a short duration from symptom occurrence to treatment (p = 0.03) and younger patient age (p = 0.038) were statistically significant factors benefiting symptom improvement, and shrinkage of the aneurysm was associated with favorable clinical outcomes (p = 0.006). Conclusions: Use of the FD with adjunctive loose coil embolization might help to alleviate the compressional symptoms caused by intracranial aneurysms. Shrinkage of the aneurysm, a short duration of symptoms, and younger patient age might contribute to favorable outcomes of mass effect-related symptoms.
Keywords: aneurysm; coil embolization; endovsacular therapy; flow diverter (FD); mass effect.
Copyright © 2019 Wang, Tian, Li, Wang, Zhu, Zhang, Zhang, Liu, Wang, Zhang and Yang.
Figures
References
LinkOut - more resources
Full Text Sources