

WSES consensus conference guidelines: monitoring and management of severe adult traumatic brain injury patients with polytrauma in the first 24 hours
- PMID: 31798673
- PMCID: PMC6884766
- DOI: 10.1186/s13017-019-0270-1
WSES consensus conference guidelines: monitoring and management of severe adult traumatic brain injury patients with polytrauma in the first 24 hours
Abstract
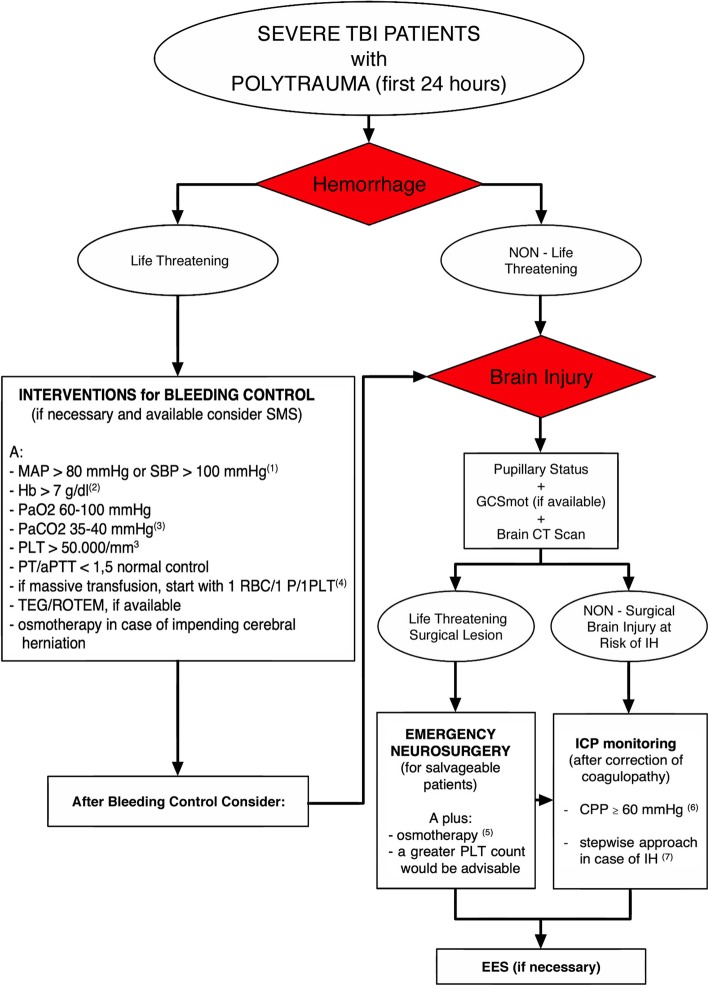
The acute phase management of patients with severe traumatic brain injury (TBI) and polytrauma represents a major challenge. Guidelines for the care of these complex patients are lacking, and worldwide variability in clinical practice has been documented in recent studies. Consequently, the World Society of Emergency Surgery (WSES) decided to organize an international consensus conference regarding the monitoring and management of severe adult TBI polytrauma patients during the first 24 hours after injury. A modified Delphi approach was adopted, with an agreement cut-off of 70%. Forty experts in this field (emergency surgeons, neurosurgeons, and intensivists) participated in the online consensus process. Sixteen recommendations were generated, with the aim of promoting rational care in this difficult setting.
Keywords: Bleeding; Hemorrhage; Management; Monitoring; Polytrauma; Traumatic brain injury.
© The Author(s). 2019.
Conflict of interest statement
Competing interestsAWK has consulted for the Innovative Trauma Care and Acelity Corporations. PFS is the co-inventor of the US patent no. 11.441.828 entitled: “Inhibition of the alternative complement pathway for treatment of traumatic brain injury, spinal cord injury, and related conditions.” All other authors declare that they have no competing interests.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study2010. Lancet. 2012;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Callcut RA, Kornblith LZ, Conroy AS, Robles AJ, Meizoso JP, Namias N, et al. Western Trauma Association Multicenter Study Group. The why and how our trauma patients die: a prospective Multicenter Western Trauma Association study. J Trauma Acute Care Surg. 2019;86(5):864–870. doi: 10.1097/TA.0000000000002205. - DOI - PMC - PubMed
