

Antidiabetic medication use during pregnancy: an international utilization study
- PMID: 31798900
- PMCID: PMC6861111
- DOI: 10.1136/bmjdrc-2019-000759
Antidiabetic medication use during pregnancy: an international utilization study
Abstract
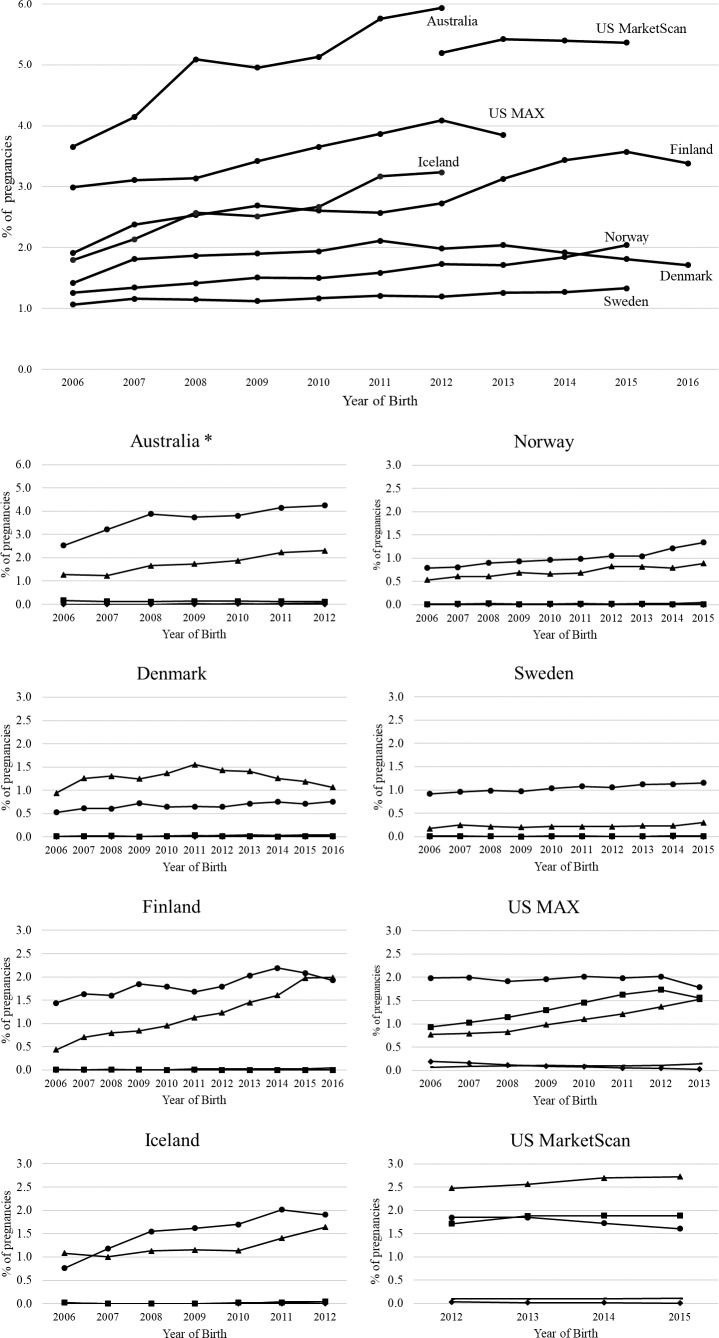
Objective: Diabetes in pregnancy and consequently the need for treatment with antidiabetic medication (ADM) has become increasingly prevalent. The prevalence and patterns of use of ADM in pregnancy from 2006 onward in seven different countries was assessed.
Research design and methods: Data sources included individually linked data from the nationwide health registers in Denmark (2006-2016), Finland (2006-2016), Iceland (2006-2012), Norway (2006-2015), Sweden (2006-2015), state-wide administrative and claims data for New South Wales, Australia (2006-2012) and two US insurance databases: Medicaid Analytic eXtract (MAX; 2006-2012, public) and IBM MarketScan (2012-2015, private). The prevalence of ADM use was calculated as the proportion of pregnancies with at least one filled prescription of an ADM in the 90 days before pregnancy or within the three trimesters of pregnancy.
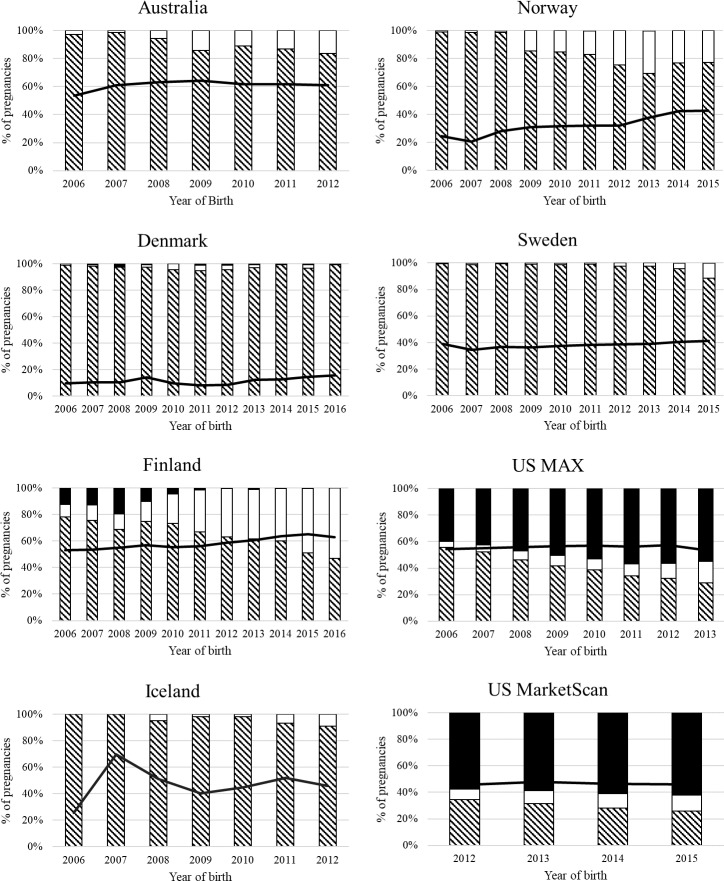
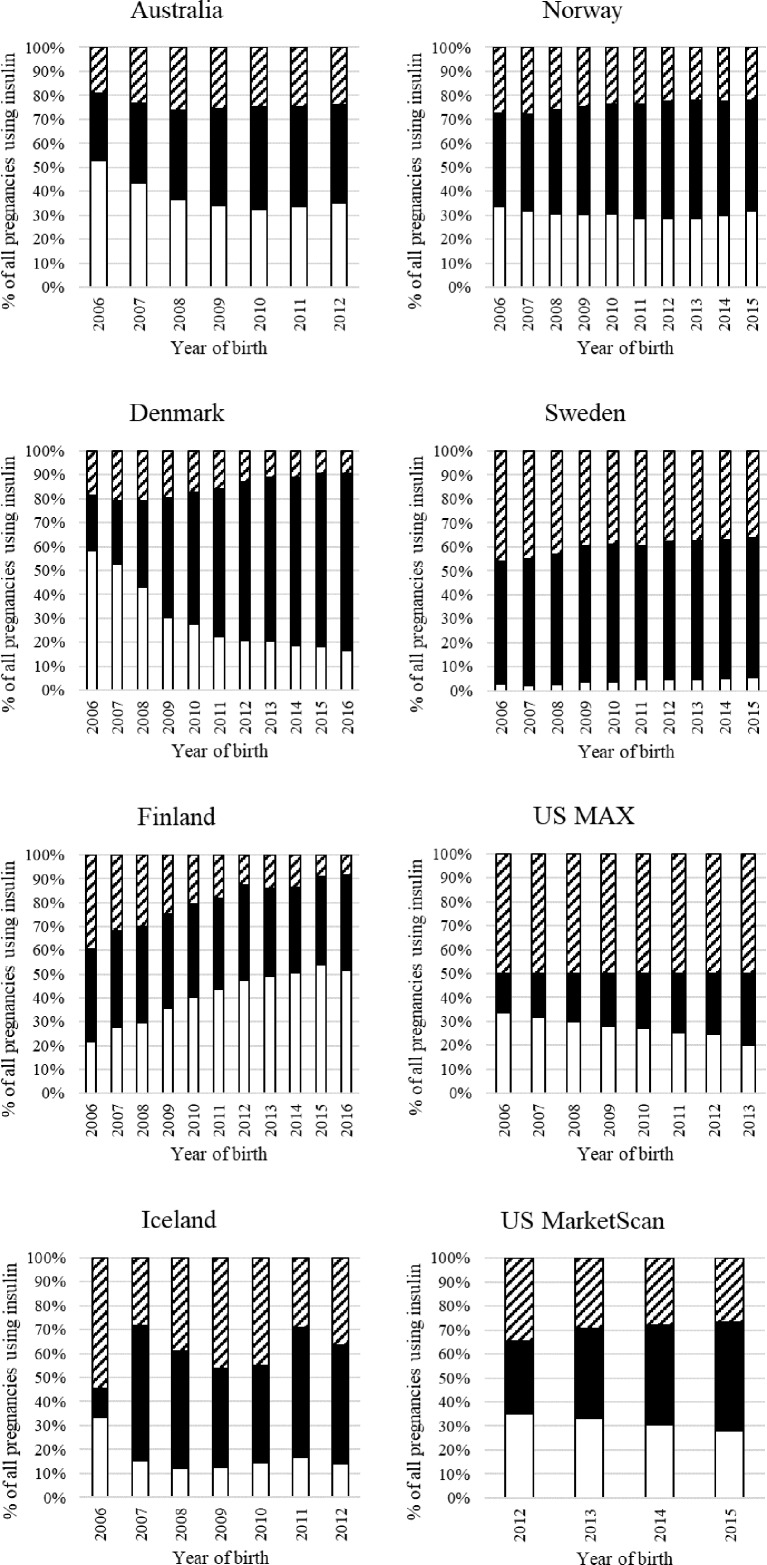
Results: Prevalence of any ADM use in 5 279 231 pregnancies was 3% (n=147 999) and varied from under 2% (Denmark, Norway, and Sweden) to above 5% (Australia and US). Insulin was the most used ADM, and metformin was the most used oral hypoglycemic agent with increasing use over time in all countries. In 11.4%-62.5% of pregnancies with prepregnancy use, ADM (primarily metformin) was discontinued. When ADM treatment was initiated in late pregnancy for treatment of gestational diabetes mellitus, insulin was most often dispensed, except in the US, where glibenclamide was most often used.
Conclusions: Prevalence and patterns of use of ADM classes varied between countries and over time. While insulin remained the most common ADM used in pregnancy, metformin use increased significantly over the study period.
Keywords: drug utilization; gestational diabetes mellitus; insulin; oral antidiabetics; pharmacoepidemiology; population-based studies; pregestational diabetes; pregnancy.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CEC, GB, HK, LP, and IO are employees at the Centre for Pharmacoepidemiology, which receives grants from several entities (pharmaceutical companies, regulatory authorities and contract research organizations) for the performance of drug safety and drug utilization studies, unrelated to this work. HLG reports fees and grants from pharmaceutical companies in her previous position at Oslo University Hospital, unrelated to this work. SH-D reports receiving research grants to her institution from Eli Lilly, GlaxoSmithKline, and the National Institutes of Health and consulting fees from Roche unrelated to this work and having served as an epidemiologist with the North America AED pregnancy registry, which is funded by multiple companies. KFH reports receiving research grants to her institution from Eli Lilly, Pfizer, GlaxoSmithKline, and Boehringer-Ingelheim, unrelated to this work. BTB reports receiving grants to his institution from Eli Lilly, GlaxoSmithKline, Pacira, Baxalta, Pfizer, and Aetion unrelated to this work and having served on an expert panel for a postpartum hemorrhage quality improvement project that was conducted by the Association of Women’s Health, Obstetric, and Neonatal Nurses and funded by a grant from Merck for Mothers. All other authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical