

Community-driven development of a modified progression-free survival ratio for precision oncology
- PMID: 31798980
- PMCID: PMC6863673
- DOI: 10.1136/esmoopen-2019-000583
Community-driven development of a modified progression-free survival ratio for precision oncology
Erratum in
-
Correction: Community-driven development of a modified progression-free survival ratio for precision oncology.ESMO Open. 2020;5(1):e000583corr1. doi: 10.1136/esmoopen-2019-000583corr1. Epub 2020 Sep 30. ESMO Open. 2020. PMID: 33551065 Free PMC article. No abstract available.
Abstract
Objective: Measuring the success of molecularly guided therapies is a major challenge in precision oncology trials. A commonly used endpoint is an intra-patient progression-free survival (PFS) ratio, defined as the PFS interval associated with molecularly guided therapy (PFS2) divided by the PFS interval associated with the last prior systemic therapy (PFS1), above 1.3 or, in some studies, above 1.33 or 1.5.
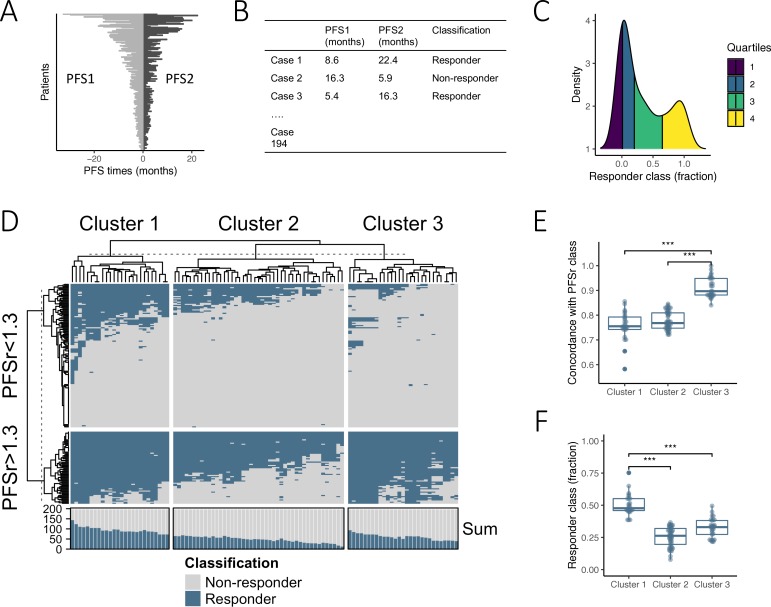
Methods: To investigate if the concept of PFS ratios is in agreement with actual response evaluations by physicians, we conducted a survey among members of the MASTER (Molecularly Aided Stratification for Tumor Eradication Research) Programme of the German Cancer Consortium who were asked to classify the success of molecularly guided therapies in 194 patients enrolled in the MOSCATO 01 trial based on PFS1 and PFS2 times.
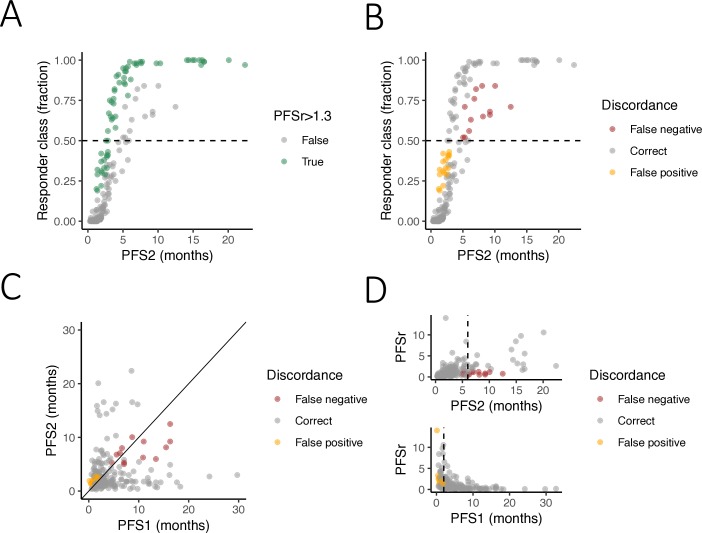
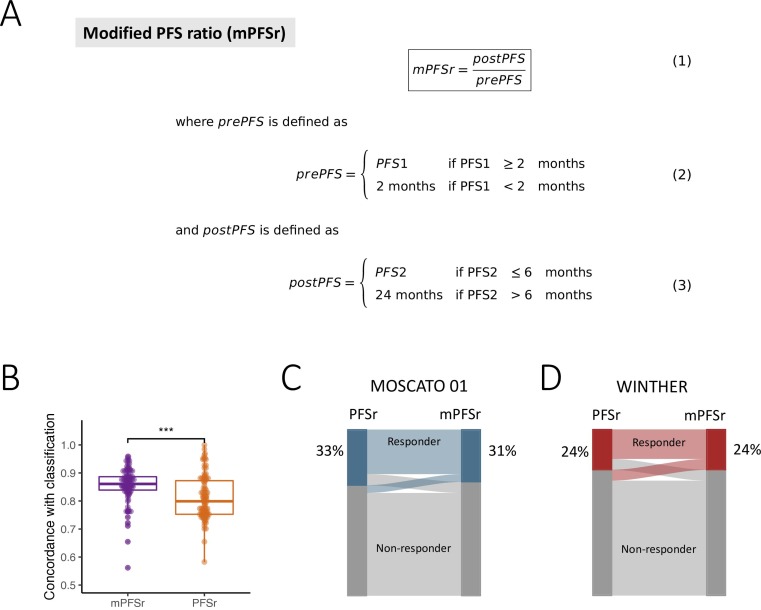
Results: A comparison of classification profiles revealed three distinct clusters of PFS benefit assessments. Only 29% of assessments were consistent with a PFS ratio threshold of 1.3, whereas the remaining 71% of participants applied a different classification scheme that did not rely on the relation between PFS times alone, but also took into account absolute PFS1 intervals. Based on these community-driven insights, we developed a modified PFS ratio that incorporates the influence of absolute PFS1 intervals on the judgement of clinical benefit by physicians. Application of the modified PFS ratio to outcome data from two recent precision oncology trials, MOSCATO 01 and WINTHER, revealed significantly improved concordance with physician-perceived clinical benefit and identified comparable proportions of patients who benefited from molecularly guided therapies.
Conclusions: The modified PFS ratio may represent a meaningful clinical endpoint that could aid in the design and interpretation of future precision oncology trials.
Keywords: N-of-1 clinical trials; PFS; personalized oncology.
© Author (s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ on behalf of the European Society for Medical Oncology.
Conflict of interest statement
Competing interests: SF has had a consulting or advisory role, received honoraria, research funding, and/or travel/accommodation expenses from the following for-profit companies: Bayer, Roche, Amgen, Eli Lilly, PharmaMar, AstraZeneca, and Pfizer.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
