

Exercise-based rehabilitation for major non-communicable diseases in low-resource settings: a scoping review
- PMID: 31798993
- PMCID: PMC6861093
- DOI: 10.1136/bmjgh-2019-001833
Exercise-based rehabilitation for major non-communicable diseases in low-resource settings: a scoping review
Abstract
Introduction: While there is substantial evidence for the benefits of exercise-based rehabilitation in the prevention and management of non-communicable disease (NCD) in high-resource settings, it is not evident that these programmes can be effectively implemented in a low-resource setting (LRS). Correspondingly, it is unclear if similar benefits can be obtained. The objective of this scoping review was to summarise existing studies evaluating exercise-based rehabilitation, rehabilitation intervention characteristics and outcomes conducted in an LRS for patients with one (or more) of the major NCDs.
Methods: The following databases were searched from inception until October 2018: PubMed/Medline, Embase, CINAHL, Cochrane Library, PsycINFO and trial registries. Studies on exercise-based rehabilitation for patients with cardiovascular disease, diabetes, cancer or chronic respiratory disease conducted in an LRS were included. Data were extracted with respect to study design (eg, type, patient sample, context), rehabilitation characteristics (eg, delivery model, programme adaptations) and included outcome measures.
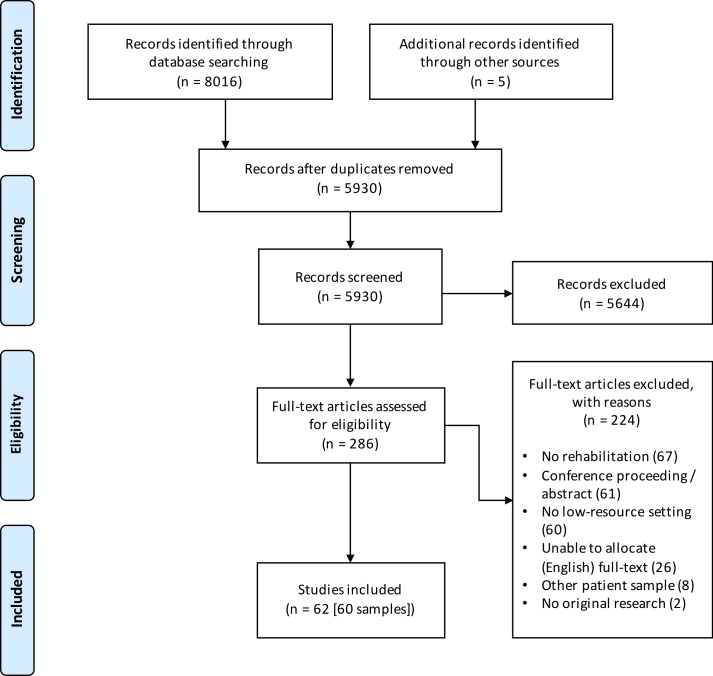
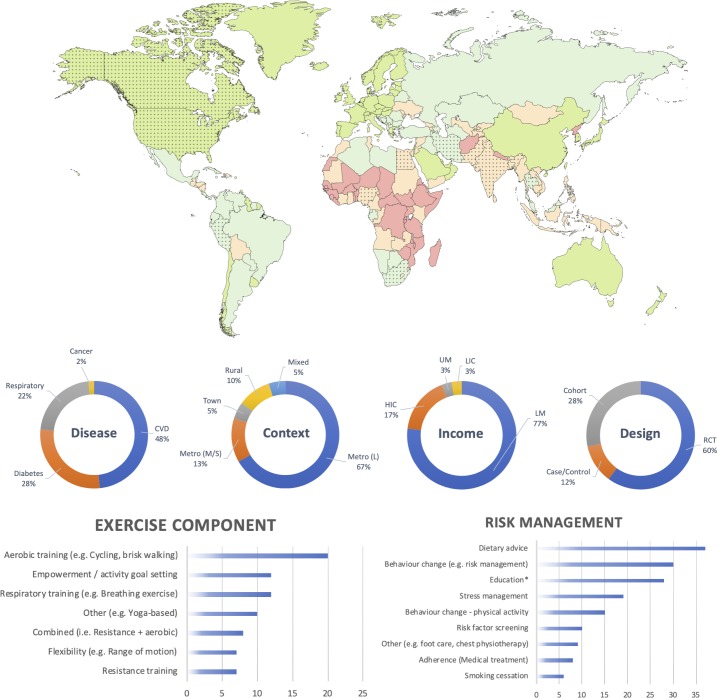
Results: The search yielded 5930 unique citations of which 60 unique studies were included. Study populations included patients with cardiovascular disease (48.3%), diabetes (28.3%), respiratory disease (21.7%) and cancer (1.7%). Adaptations included transition to predominant patient-driven home-based rehabilitation, training of non-conventional health workers, integration of rehabilitation in community health centres, or triage based on contextual or patient factors. Uptake of adapted rehabilitation models was 54%, retention 78% and adherence 89%. The majority of the outcome measures included were related to body function (65.7%).
Conclusions: The scope of evidence suggests that adapted exercise-based rehabilitation programmes can be implemented in LRS. However, this scope of evidence originated largely from lower middle-income, urban settings and has mostly been conducted in an academic context which may hamper extrapolation of evidence to other LRS. Cost-benefits, impact on activity limitations and participation restrictions, and subsequent mortality and morbidity are grossly understudied.
Keywords: developing countries; noncommunicable disease; rehabilitation.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO Global status report on noncommunicable diseases, 2014. Available: http://www.who.int/nmh/publications/ncd-status-report-2014/en/ [Accessed 25 Jun 2018].
Publication types
LinkOut - more resources
Full Text Sources