

Hyperkalemia: pathophysiology, risk factors and consequences
- PMID: 31800080
- PMCID: PMC6892421
- DOI: 10.1093/ndt/gfz206
Hyperkalemia: pathophysiology, risk factors and consequences
Abstract
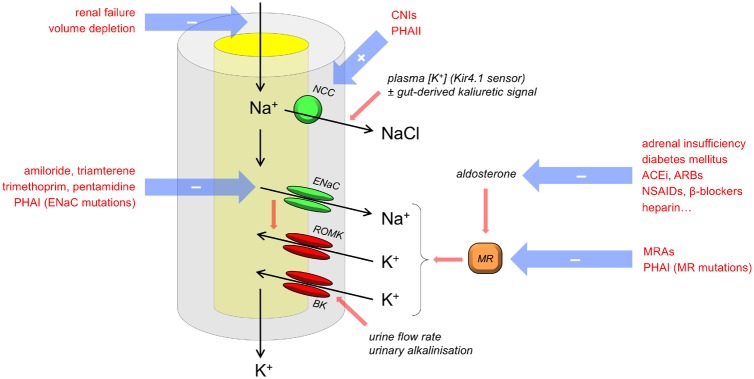
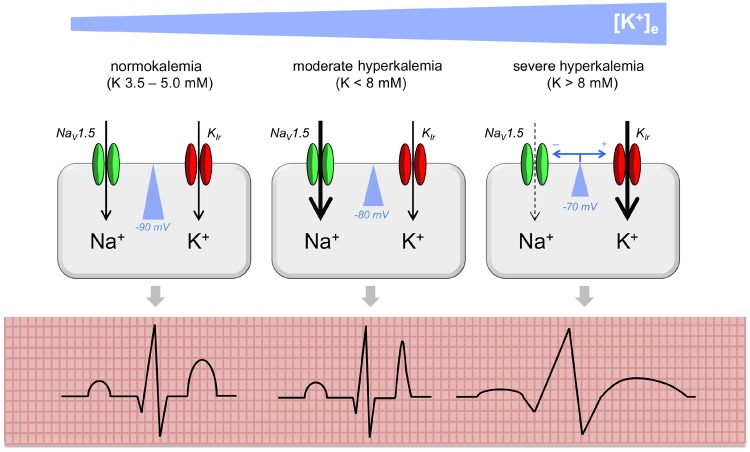
There have been significant recent advances in our understanding of the mechanisms that maintain potassium homoeostasis and the clinical consequences of hyperkalemia. In this article we discuss these advances within a concise review of the pathophysiology, risk factors and consequences of hyperkalemia. We highlight aspects that are of particular relevance for clinical practice. Hyperkalemia occurs when renal potassium excretion is limited by reductions in glomerular filtration rate, tubular flow, distal sodium delivery or the expression of aldosterone-sensitive ion transporters in the distal nephron. Accordingly, the major risk factors for hyperkalemia are renal failure, diabetes mellitus, adrenal disease and the use of angiotensin-converting enzyme inhibitors, angiotensin receptor blockers or potassium-sparing diuretics. Hyperkalemia is associated with an increased risk of death, and this is only in part explicable by hyperkalemia-induced cardiac arrhythmia. In addition to its well-established effects on cardiac excitability, hyperkalemia could also contribute to peripheral neuropathy and cause renal tubular acidosis. Hyperkalemia-or the fear of hyperkalemia-contributes to the underprescription of potentially beneficial medications, particularly in heart failure. The newer potassium binders could play a role in attempts to minimize reduced prescribing of renin-angiotensin inhibitors and mineraolocorticoid antagonists in this context.
Keywords: aldosterone; arrhythmia; hyperkalemia; potassium; renin–angiotensin.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Eaton SB, Konner M.. Paleolithic nutrition. A consideration of its nature and current implications. N Engl J Med 1985; 312: 283–289 - PubMed
-
- Preston RA, Afshartous D, Rodco R. et al. Evidence for a gastrointestinal–renal kaliuretic signaling axis in humans. Kidney Int 2015; 88: 1383–1391 - PubMed
-
- Rabinowitz L, Green DM, Sarason RL. et al. Homeostatic potassium excretion in fed and fasted sheep. Am J Physiol 1988; 254: R357–380 - PubMed
-
- Lee FN, Oh G, McDonough AA, Youn JH.. Evidence for gut factor in K+ homeostasis. Renal Physiol 2007; 293: F541-F547 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
