

Hip Joint Capsular Anatomy, Mechanics, and Surgical Management
- PMID: 31800428
- PMCID: PMC7406151
- DOI: 10.2106/JBJS.19.00346
Hip Joint Capsular Anatomy, Mechanics, and Surgical Management
Abstract
- ➤
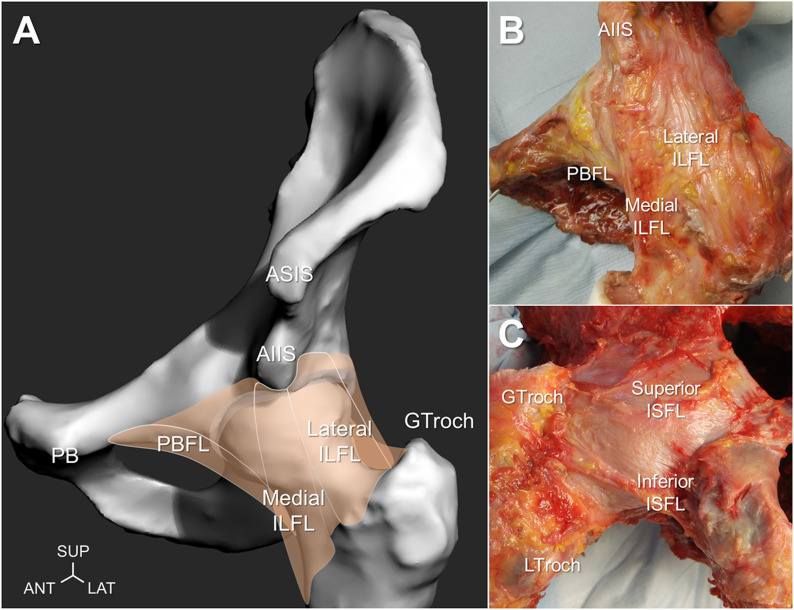
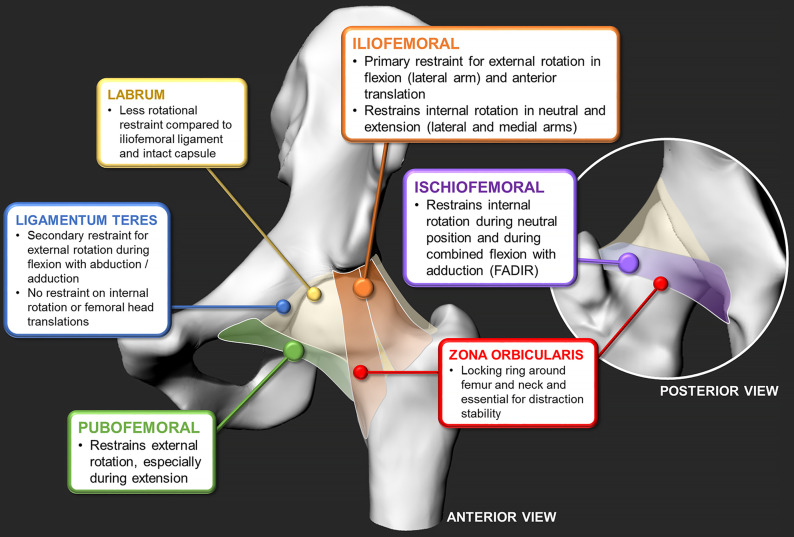
Hip joint capsular ligaments (iliofemoral, ischiofemoral, and pubofemoral) play a predominant role in functional mobility and joint stability.
- ➤
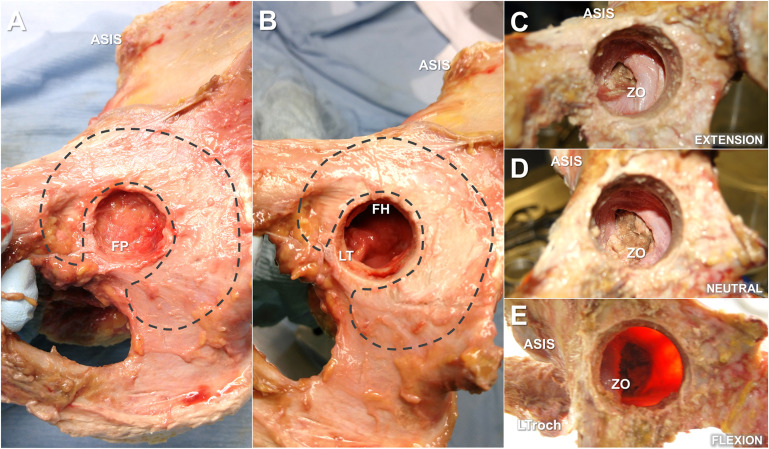
The zona orbicularis resists joint distraction (during neutral positions), and its aperture mechanism stabilizes the hip from adverse edge-loading (during extreme hip flexion-extension).
- ➤
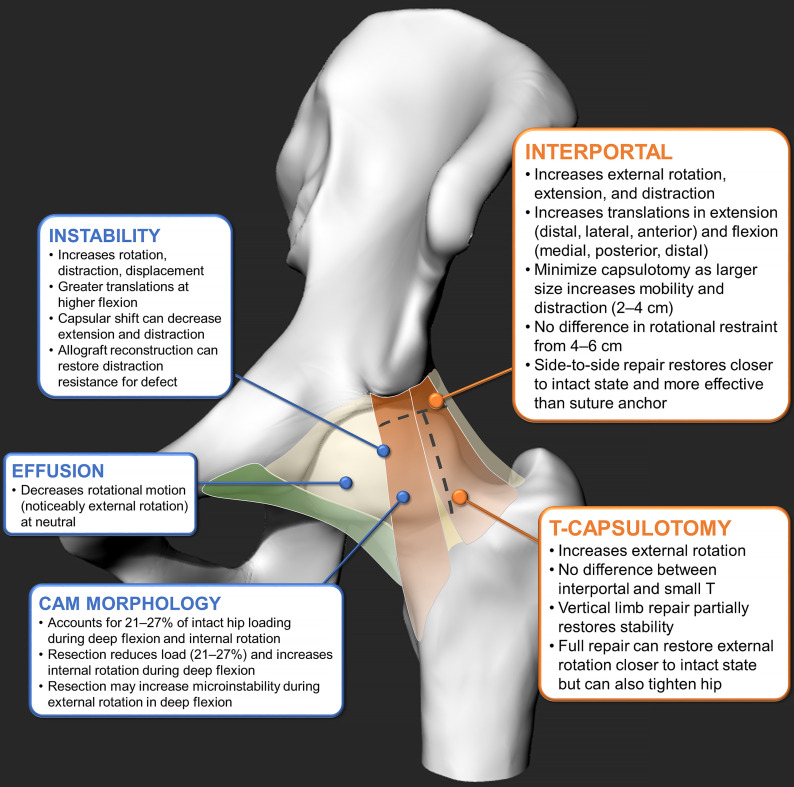
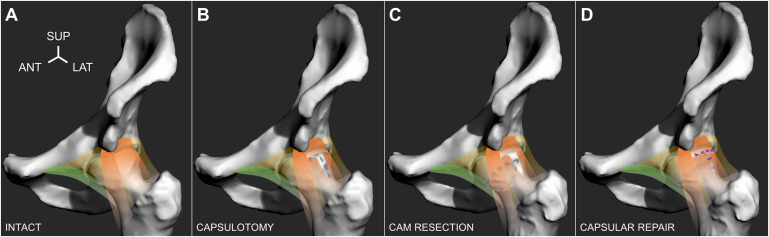
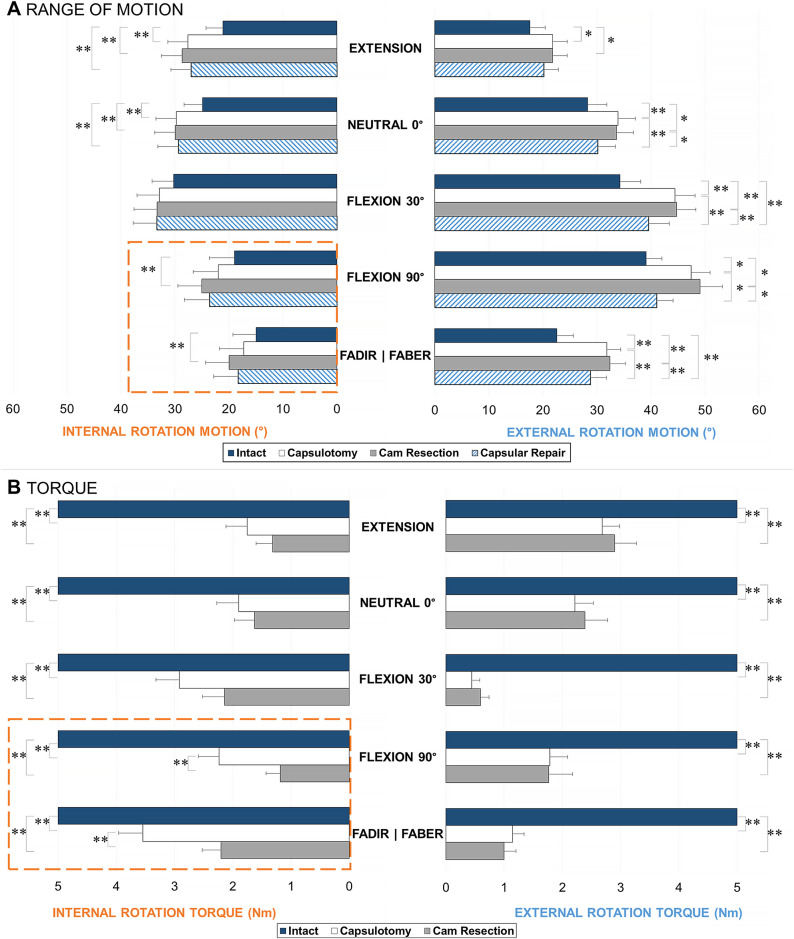
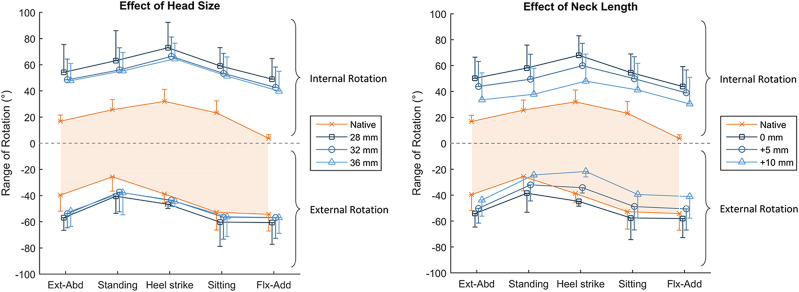
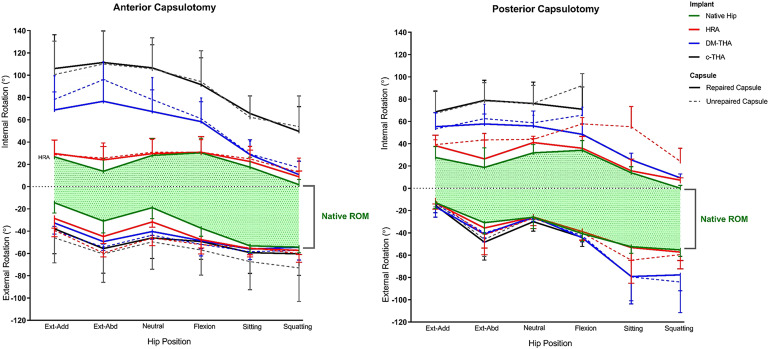
To preserve joint function and stability, it is important to minimize capsulotomy size and avoid disrupting the zona orbicularis, preserve the femoral head size and neck length, and only repair when or as necessary without altering capsular tensions.
- ➤
It is not fully understood what the role of capsular tightness is in patients who have cam femoroacetabular impingement and if partial capsular release could be beneficial and/or therapeutic.
- ➤
During arthroplasty surgery, a femoral head implant that is nearly equivalent to the native head size with an optimal neck-length offset can optimize capsular tension and decrease dislocation risk where an intact posterior hip capsule plays a critical role in maintaining hip stability.
Figures
References
-
- Hewitt J, Guilak F, Glisson R, Vail TP. Regional material properties of the human hip joint capsule ligaments. J Orthop Res. 2001. May;19(3):359-64. - PubMed
-
- Malagelada F, Tayar R, Barke S, Stafford G, Field RE. Anatomy of the zona orbicularis of the hip: a magnetic resonance study. Surg Radiol Anat. 2015. January;37(1):11-8. Epub 2014 Apr 29. - PubMed
-
- Wagner FV, Negrão JR, Campos J, Ward SR, Haghighi P, Trudell DJ, Resnick D. Capsular ligaments of the hip: anatomic, histologic, and positional study in cadaveric specimens with MR arthrography. Radiology. 2012. April;263(1):189-98. Epub 2012 Feb 27. - PubMed
-
- Walters BL, Cooper JH, Rodriguez JA. New findings in hip capsular anatomy: dimensions of capsular thickness and pericapsular contributions. Arthroscopy. 2014. October;30(10):1235-45. Epub 2014 Jul 23. - PubMed
-
- Bedi A, Galano G, Walsh C, Kelly BT. Capsular management during hip arthroscopy: from femoroacetabular impingement to instability. Arthroscopy. 2011. December;27(12):1720-31. Epub 2011 Nov 1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
