

Incidental Congestive Heart Failure in Patients With Aldosterone-Producing Adenomas
- PMID: 31801414
- PMCID: PMC6951059
- DOI: 10.1161/JAHA.119.012410
Incidental Congestive Heart Failure in Patients With Aldosterone-Producing Adenomas
Abstract
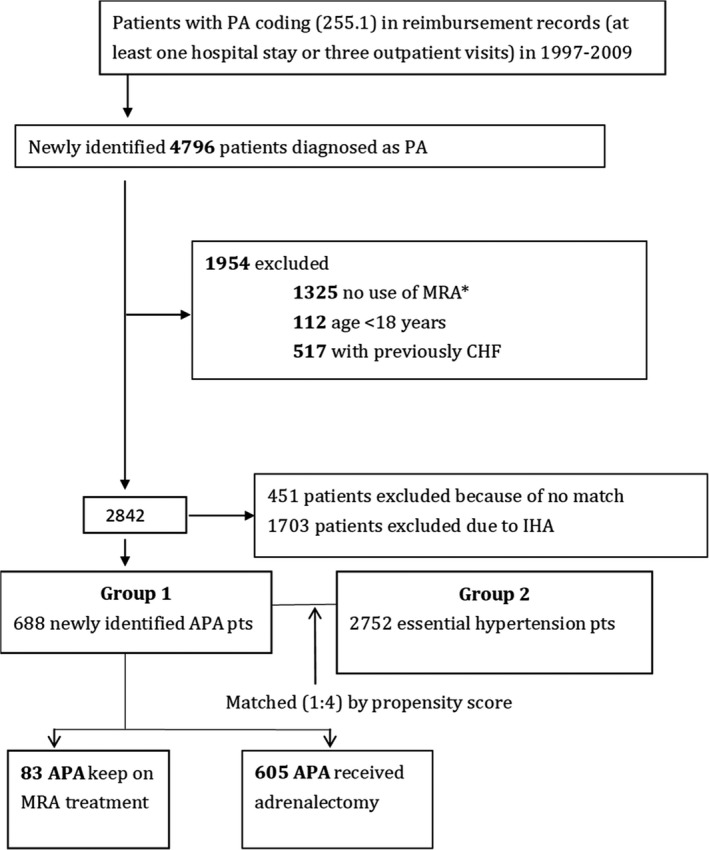
Background Previous studies show that patients with primary aldosteronism are associated with higher risk of congestive heart failure (CHF). However, the effect of target treatment to the incidental CHF has not been elucidated. We aimed to investigate the risk of new-onset CHF in patients with aldosterone-producing adenomas (APAs) and explore the effect of adrenalectomy on new onset of CHF. Methods and Results From 1997 to 2009, 688 APA were identified and matched with essential hypertension controls. The risks of developing incidental CHF (hazard ratio, 0.49; 95% CI, 0.31-0.75; P=0.001) and mortality (hazard ratio, 0.29; 95% CI, 0.20-0.44; P<0.001) were significantly lower in the APA group after targeted treatment. A total of 605 patients with APAs who underwent adrenalectomy lowered the risks of CHF (subdistribution hazard ratio, 0.55; 95% CI, 0.34-0.90; P=0.017) and mortality (adjusted hazard ratio, 0.27; 95% CI, 0.16-0.44; P<0.001) compared with essential hypertension controls. Conclusions In conclusion, for patients with APAs, adrenalectomy can be associated with lower risk of incidental CHF and all-cause mortality in a long-term follow-up.
Keywords: adrenalectomy; aldosterone‐producing adenomas; cardiovascular disease; congestive heart failure; essential hypertension; primary aldosteronism.
Figures
References
-
- Monticone S, Burrello J, Tizzani D, Bertello C, Viola A, Buffolo F, Gabetti L, Mengozzi G, Williams TA, Rabbia F, Veglio F, Mulatero P. Prevalence and clinical manifestations of primary aldosteronism encountered in primary care practice. J Am Coll Cardiol. 2017;69:1811–1820. - PubMed
-
- Horton R. Aldosterone: review of its physiology and diagnostic aspects of primary aldosteronism. Metabolism. 1973;22:1525–1545. - PubMed
-
- Nicholls MG, Ramsay LE, Boddy K, Fraser R, Morton JJ, Robertson JI. Mineralocorticoid‐induced blood pressure, electrolyte, and hormone changes, and reversal with spironolactone, in healthy men. Metabolism. 1979;28:584–593. - PubMed
-
- Young WF Jr. Minireview: primary aldosteronism–changing concepts in diagnosis and treatment. Endocrinology. 2003;144:2208–2213. - PubMed
-
- Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ. Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol. 2005;45:1243–1248. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
