

Pre-arrest and intra-arrest prognostic factors associated with survival after in-hospital cardiac arrest: systematic review and meta-analysis
- PMID: 31801749
- PMCID: PMC6891802
- DOI: 10.1136/bmj.l6373
Pre-arrest and intra-arrest prognostic factors associated with survival after in-hospital cardiac arrest: systematic review and meta-analysis
Abstract
Objective: To determine associations between important pre-arrest and intra-arrest prognostic factors and survival after in-hospital cardiac arrest.
Design: Systematic review and meta-analysis.
Data sources: Medline, PubMed, Embase, Scopus, Web of Science, and the Cochrane Database of Systematic Reviews from inception to 4 February 2019. Primary, unpublished data from the United Kingdom National Cardiac Arrest Audit database.
Study selection criteria: English language studies that investigated pre-arrest and intra-arrest prognostic factors and survival after in-hospital cardiac arrest.
Data extraction: PROGRESS (prognosis research strategy group) recommendations and the CHARMS (critical appraisal and data extraction for systematic reviews of prediction modelling studies) checklist were followed. Risk of bias was assessed by using the QUIPS tool (quality in prognosis studies). The primary analysis pooled associations only if they were adjusted for relevant confounders. The GRADE approach (grading of recommendations assessment, development, and evaluation) was used to rate certainty in the evidence.
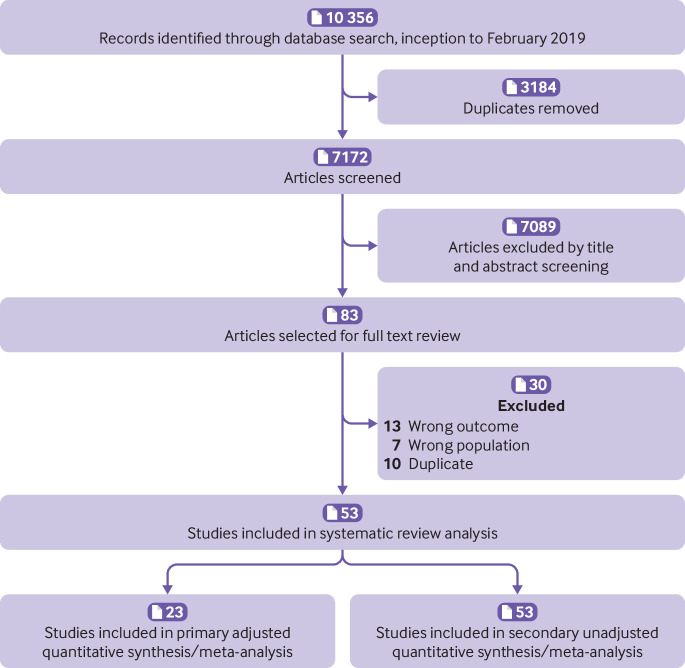
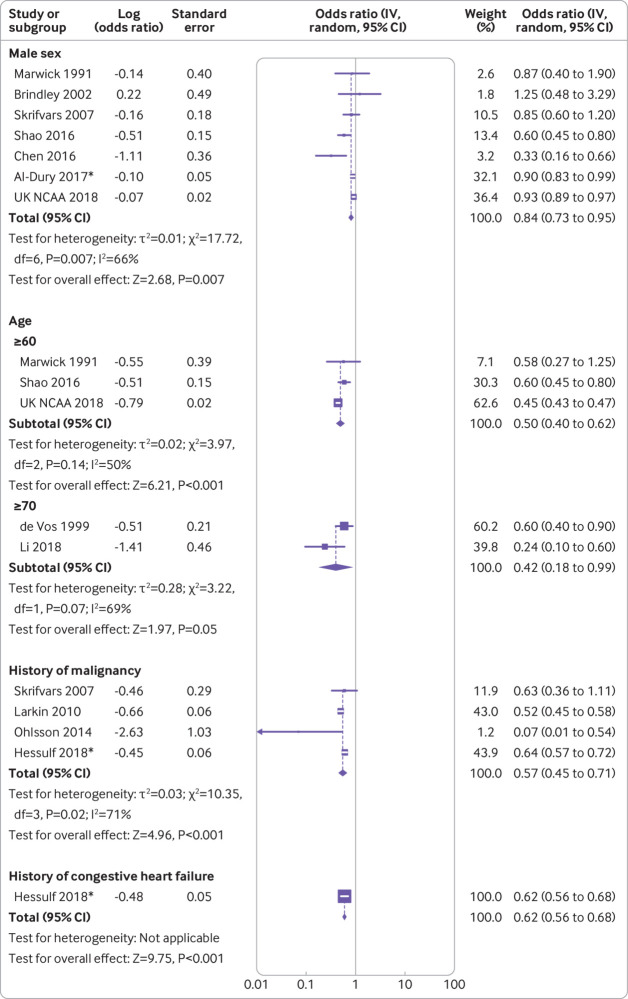
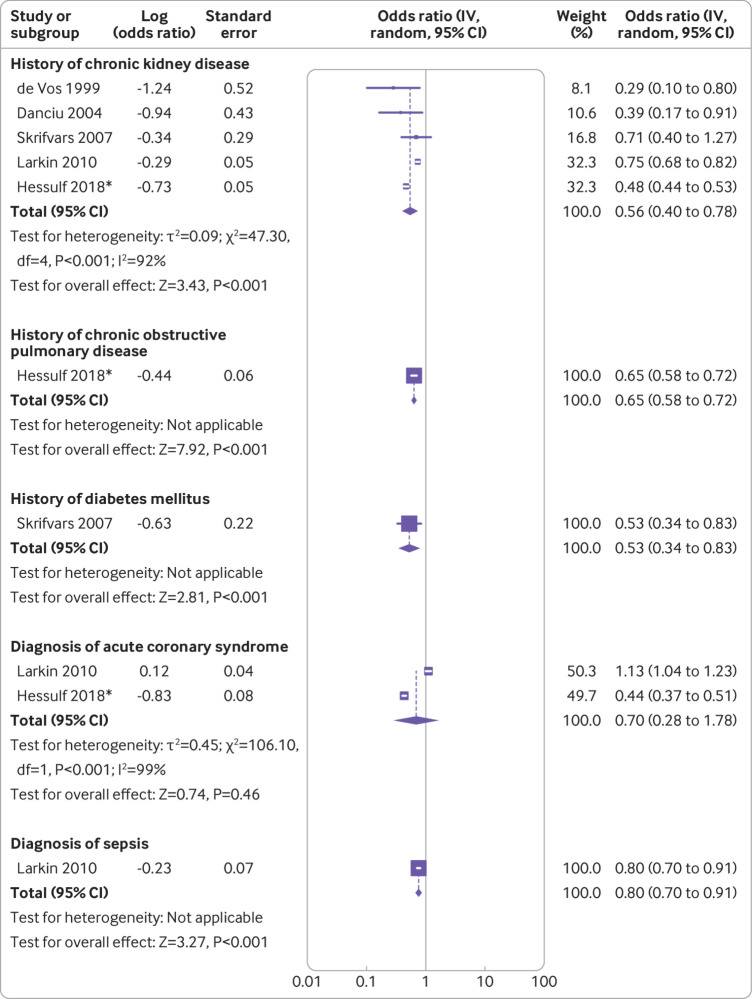
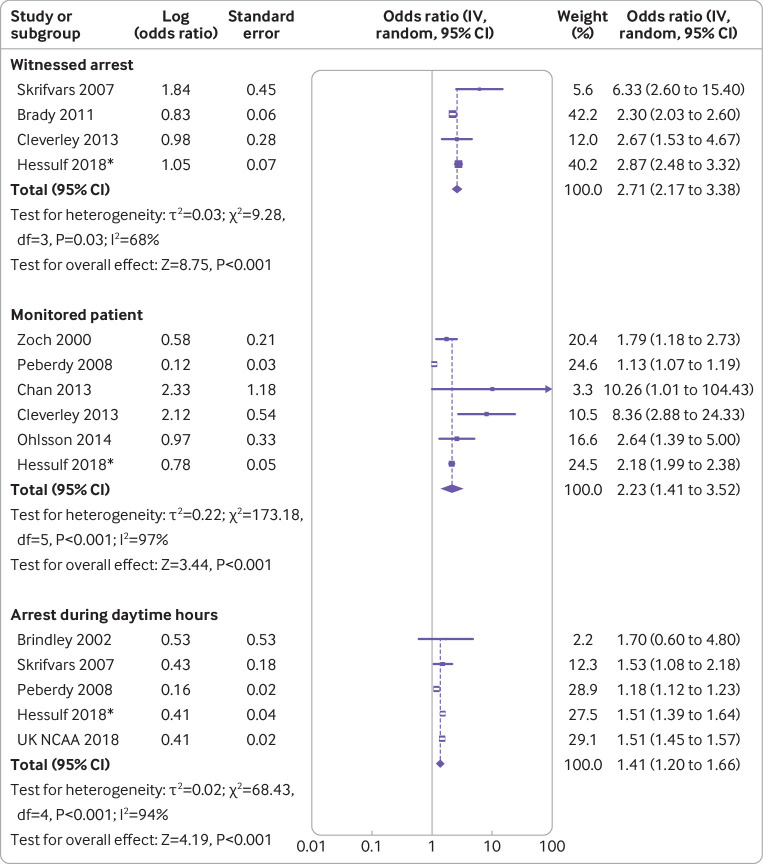
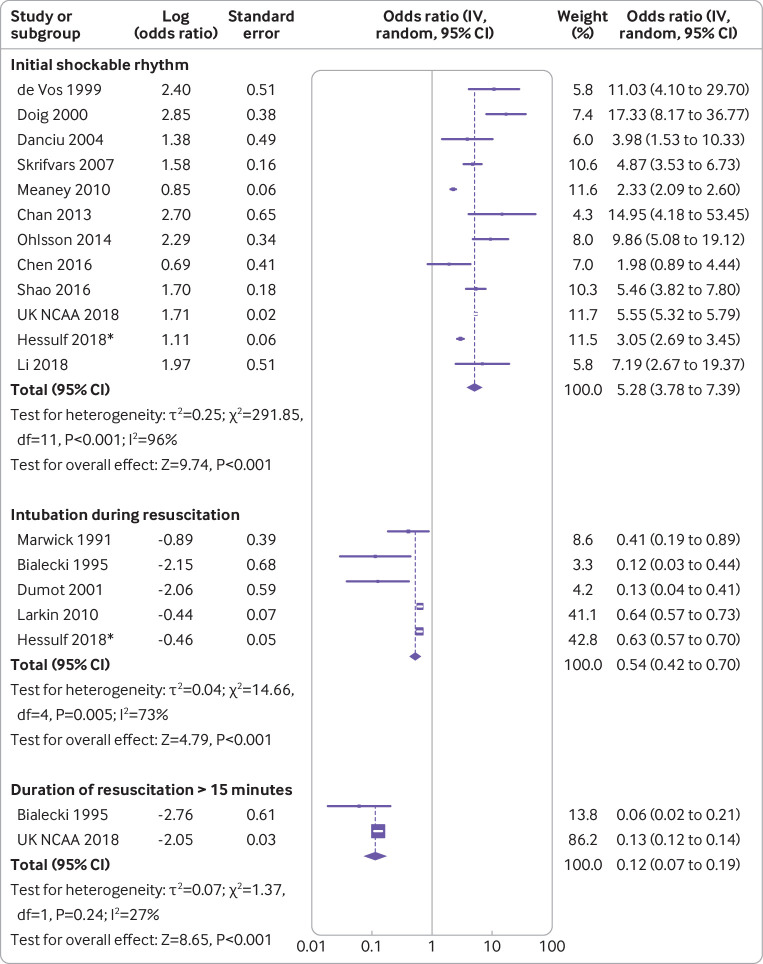
Results: The primary analysis included 23 cohort studies. Of the pre-arrest factors, male sex (odds ratio 0.84, 95% confidence interval 0.73 to 0.95, moderate certainty), age 60 or older (0.50, 0.40 to 0.62, low certainty), active malignancy (0.57, 0.45 to 0.71, high certainty), and history of chronic kidney disease (0.56, 0.40 to 0.78, high certainty) were associated with reduced odds of survival after in-hospital cardiac arrest. Of the intra-arrest factors, witnessed arrest (2.71, 2.17 to 3.38, high certainty), monitored arrest (2.23, 1.41 to 3.52, high certainty), arrest during daytime hours (1.41, 1.20 to 1.66, high certainty), and initial shockable rhythm (5.28, 3.78 to 7.39, high certainty) were associated with increased odds of survival. Intubation during arrest (0.54, 0.42 to 0.70, moderate certainty) and duration of resuscitation of at least 15 minutes (0.12, 0.07 to 0.19, high certainty) were associated with reduced odds of survival.
Conclusion: Moderate to high certainty evidence was found for associations of pre-arrest and intra-arrest prognostic factors with survival after in-hospital cardiac arrest.
Systematic review registration: PROSPERO CRD42018104795.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Morrison LJ, Neumar RW, Zimmerman JL, et al. American Heart Association Emergency Cardiovascular Care Committee, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on P Strategies for improving survival after in-hospital cardiac arrest in the United States: 2013 consensus recommendations: a consensus statement from the American Heart Association. Circulation 2013;127:1538-63. 10.1161/CIR.0b013e31828b2770. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical