

Postoperative delirium is associated with increased plasma neurofilament light
- PMID: 31802104
- PMCID: PMC6935744
- DOI: 10.1093/brain/awz354
Postoperative delirium is associated with increased plasma neurofilament light
Erratum in
-
Erratum.Brain. 2020 Mar 1;143(3):e24. doi: 10.1093/brain/awaa007. Brain. 2020. PMID: 32333675 Free PMC article. No abstract available.
Abstract
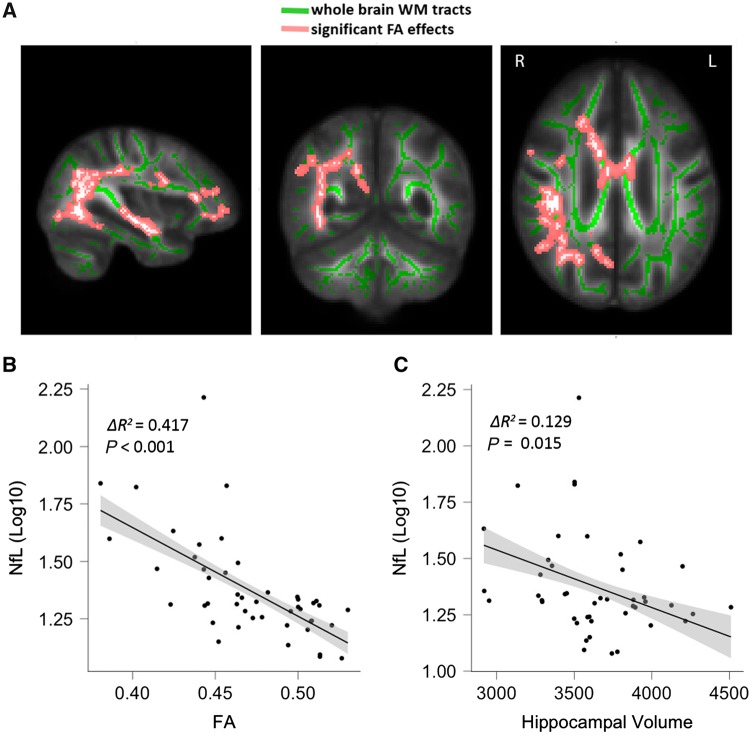
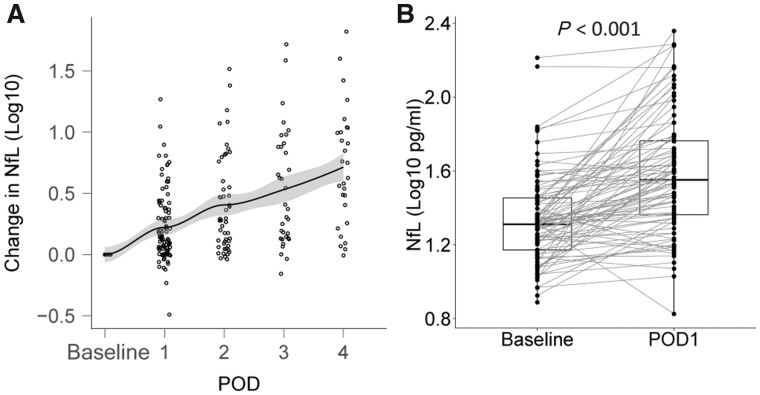
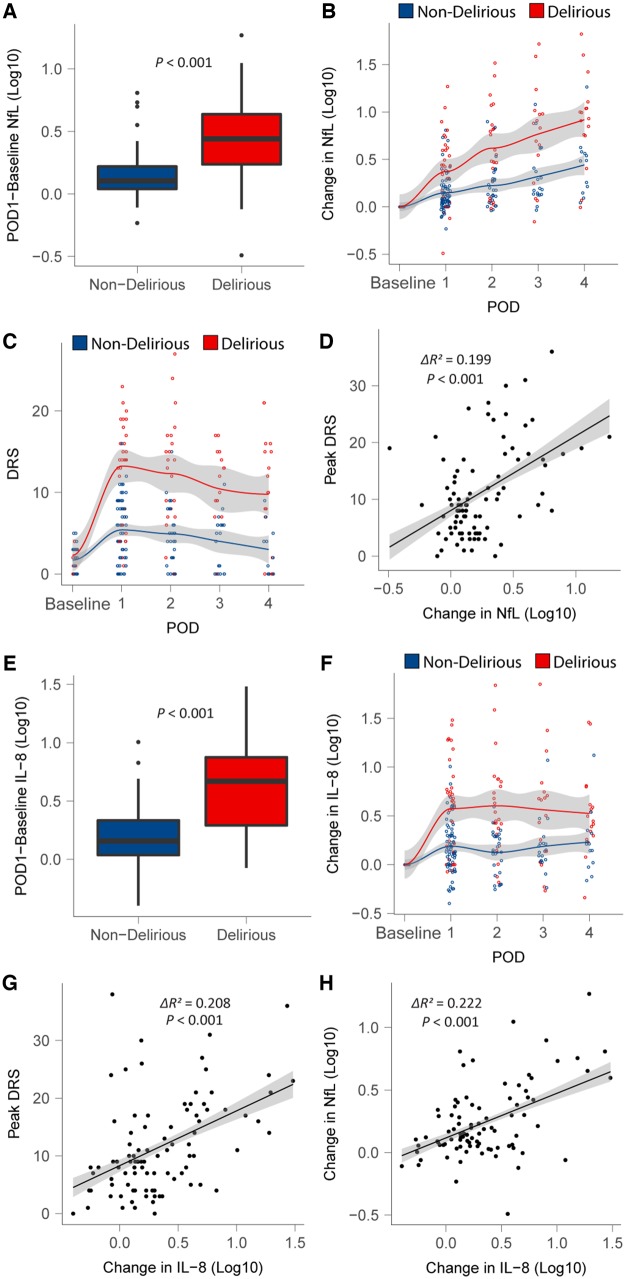
While delirium is associated with cognitive decline and dementia, there is limited evidence to support causality for this relationship. Clarification of how delirium may cause cognitive decline, perhaps through evidence of contemporaneous neuronal injury, would enhance plausibility for a causal relationship. Dose-dependence of neuronal injury with delirium severity would further enhance the biological plausibility for this relationship. We tested whether delirium is associated with neuronal injury in 114 surgical patients recruited to a prospective biomarker cohort study. Patients underwent perioperative testing for changes in neurofilament light, a neuronal injury biomarker, as well as a panel of 10 cytokines, with contemporaneous assessment of delirium severity and incidence. A subset of patients underwent preoperative MRI. Initially we confirmed prior reports that neurofilament light levels correlated with markers of neurodegeneration [hippocampal volume (ΔR2 = 0.129, P = 0.015)] and white matter changes including fractional anisotropy of white matter (ΔR2 = 0.417, P < 0.001) with similar effects on mean, axial and radial diffusivity) in our cohort and that surgery was associated with increasing neurofilament light from preoperative levels [mean difference (95% confidence interval, CI) = 0.240 (0.178, 0.301) log10 (pg/ml), P < 0.001], suggesting putative neuronal injury. Next, we tested the relationship with delirium. Neurofilament light rose more sharply in participants with delirium compared to non-sufferers [mean difference (95% CI) = 0.251 (0.136, 0.367) log10 (pg/ml), P < 0.001]. This relationship showed dose-dependence, such that neurofilament light rose proportionately to delirium severity (ΔR2 = 0.199, P < 0.001). Given that inflammation is considered an important driver of postoperative delirium, next we tested whether neurofilament light, as a potential marker of neurotoxicity, may contribute to the pathogenesis of delirium independent of inflammation. From a panel of 10 cytokines, the pro-inflammatory cytokine IL-8 exhibited a strong correlation with delirium severity (ΔR2 = 0.208, P < 0.001). Therefore, we tested whether the change in neurofilament light contributed to delirium severity independent of IL-8. Neurofilament light was independently associated with delirium severity after adjusting for the change in inflammation (ΔR2 = 0.040, P = 0.038). These data suggest delirium is associated with exaggerated increases in neurofilament light and that this putative neurotoxicity may contribute to the pathogenesis of delirium itself, independent of changes in inflammation.
Keywords: cognition; delirium; inflammation; neuronal injury; surgery.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Avants BB, Tustison N, Song G. Advanced normalization tools (ANTS). Insight j 2009; 2: 1–35.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
