

The MRI spectrum of congenital cytomegalovirus infection
- PMID: 31802515
- PMCID: PMC7027449
- DOI: 10.1002/pd.5591
The MRI spectrum of congenital cytomegalovirus infection
Abstract
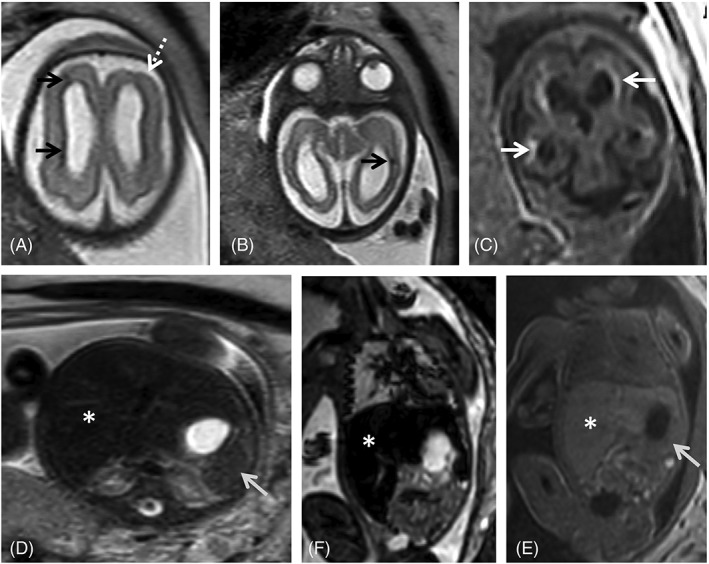
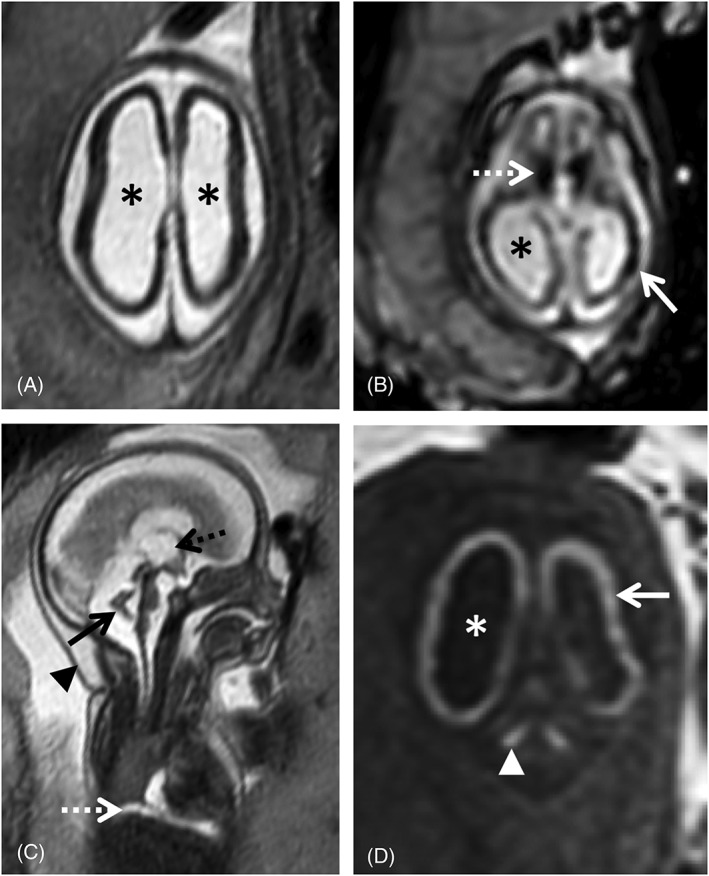
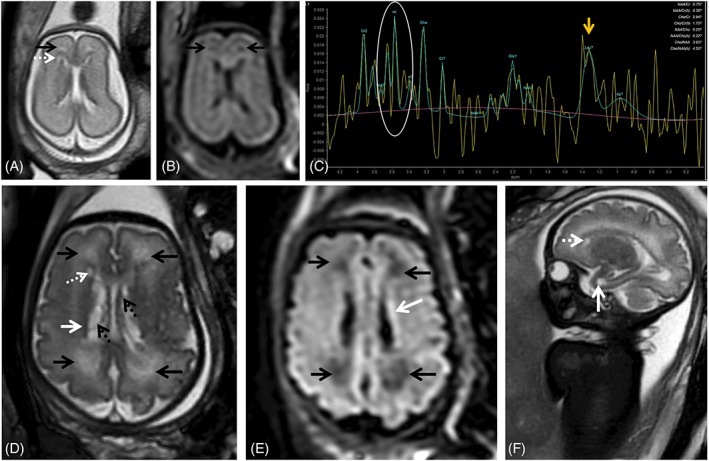
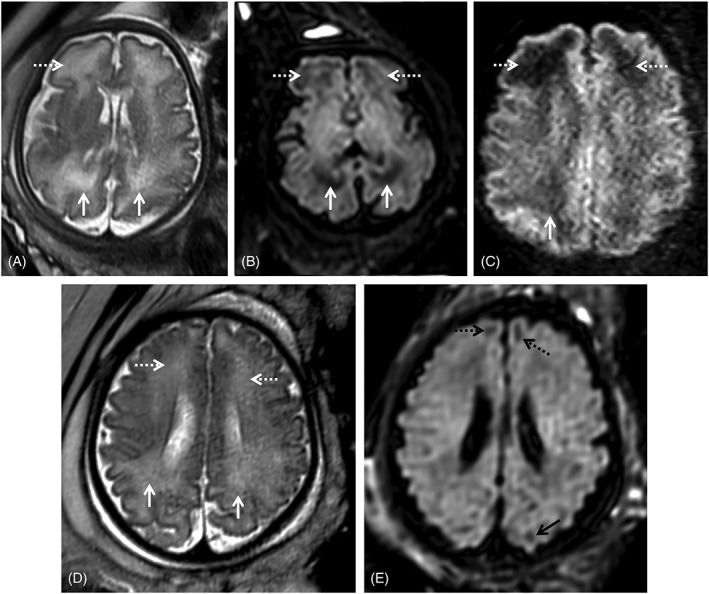
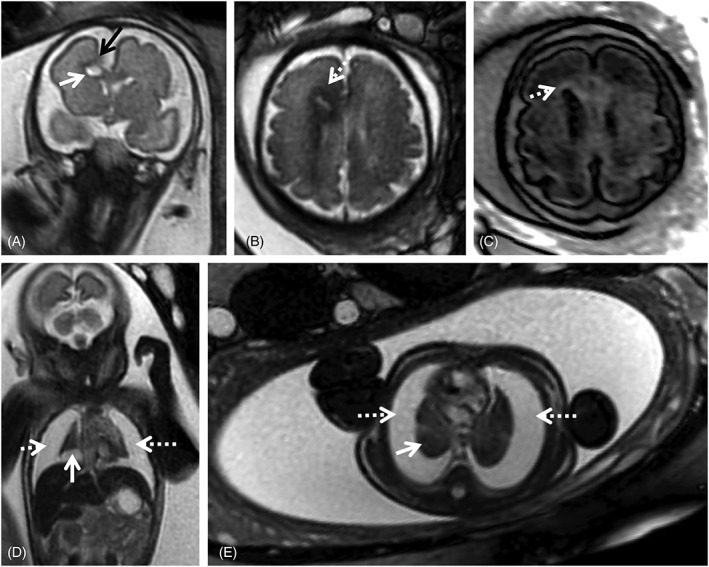
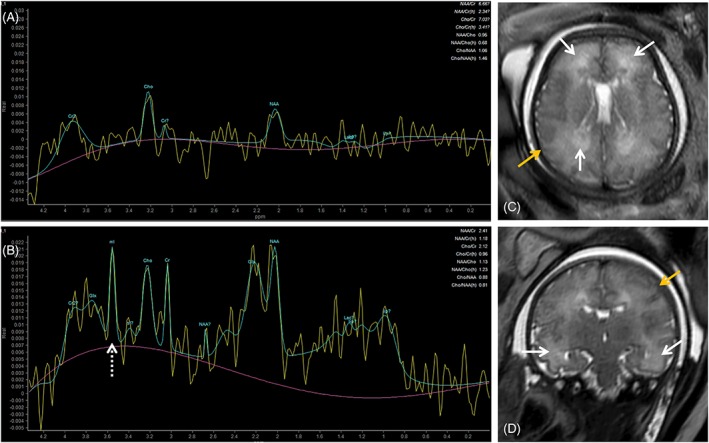
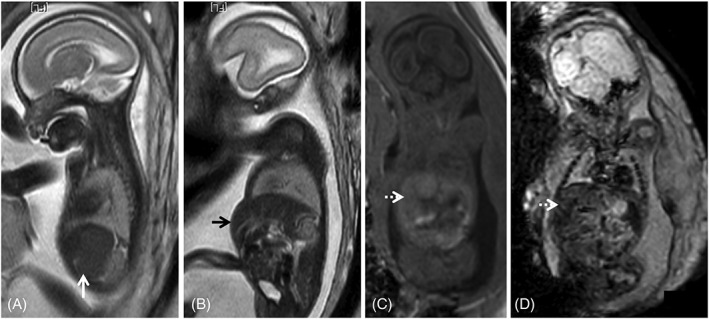
Human cytomegalovirus (CMV) is an ubiquitous pathogen, with a high worldwide seroprevalence. When acquired in the prenatal period, congenital CMV (cCMV) is a major cause of neurodevelopmental sequelae and hearing loss. cCMV remains an underdiagnosed condition, with no systematic screening implemented in pregnancy or in the postnatal period. Therefore, imaging takes a prominent role in prenatal diagnosis of cCMV. With the prospect of new viable therapies, accurate and timely diagnosis becomes paramount, as well as identification of fetuses at risk for neurodevelopmental sequelae. Fetal magnetic resonance imaging (MRI) provides a complementary method to ultrasound (US) in fetal brain and body imaging. Anterior temporal lobe lesions are the most specific finding, and MRI is superior to US in their detection. Other findings such as ventriculomegaly, cortical malformations and calcifications, as well as hepatosplenomegaly, liver signal changes and abnormal effusions are unspecific. However, when seen in combination these should raise the suspicion of fetal infection, highlighting the need for a full fetal assessment. Still, some fetuses deemed normal on prenatal imaging are symptomatic at birth or develop delayed cCMV-associated symptoms, leaving room for improvement of diagnostic tools. Advanced MR sequences may help in this field and in determining prognosis, but further studies are needed.
© 2019 The Authors. Prenatal Diagnosis published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Sert Y, Ozgu‐Erdinc AS, Saygan S, Engin UY. Antenatal cytomegalovirus infection screening results of 32,188 patients in a tertiary referral center: A retrospective cohort study. Fetal Pediatr Pathol. 2019;38(2):112‐120. - PubMed
-
- Griffiths P, Baraniak I, Reeves M. The pathogenesis of human cytomegalovirus. J Pathol. 2015;235(2):288‐297. - PubMed
-
- Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010;20(4):202‐213. - PubMed
