

Successful treatment of metastatic adrenocortical carcinoma in the spine: A case report and literature review
- PMID: 31804360
- PMCID: PMC6919434
- DOI: 10.1097/MD.0000000000018259
Successful treatment of metastatic adrenocortical carcinoma in the spine: A case report and literature review
Abstract
Rationale: Adrenocortical carcinoma is a rare aggressive type of cancer whose prognosis is poor, particularly for metastatic entities. Metastatic adrenocortical carcinoma in the spine is a rare disease with no standard curative managements yet. The objective of this study is to report a very rare case of spinal metastases of adrenocortical carcinoma successfully managed by combination of cement augmentation, radiotherapy together with adjuvant programmed cell death 1 (PD-1) therapy. The management of these unique cases has yet to be well-documented.
Patient concerns: A 42-year-old woman presented with a 3-month history of continuous and progressive back pain. The patient, who had been diagnosed of right pheochromocytoma, received surgical treatment of right adrenalectomy 14 months ago in another hospital, followed by no further treatment.
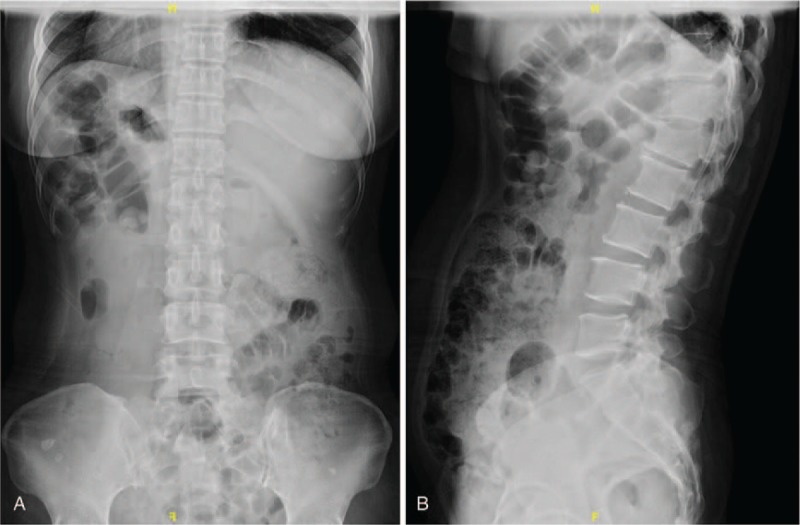
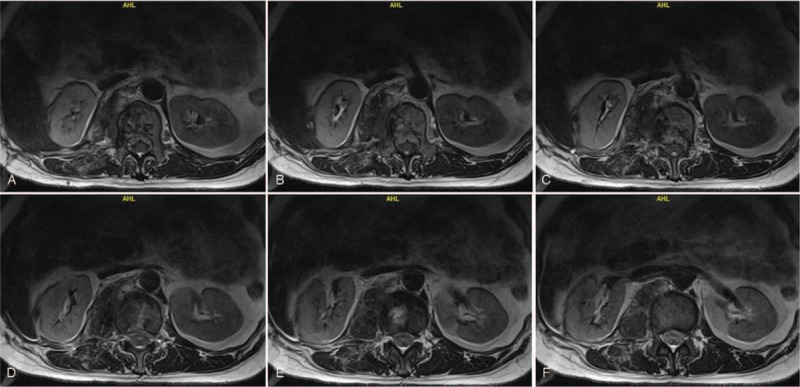
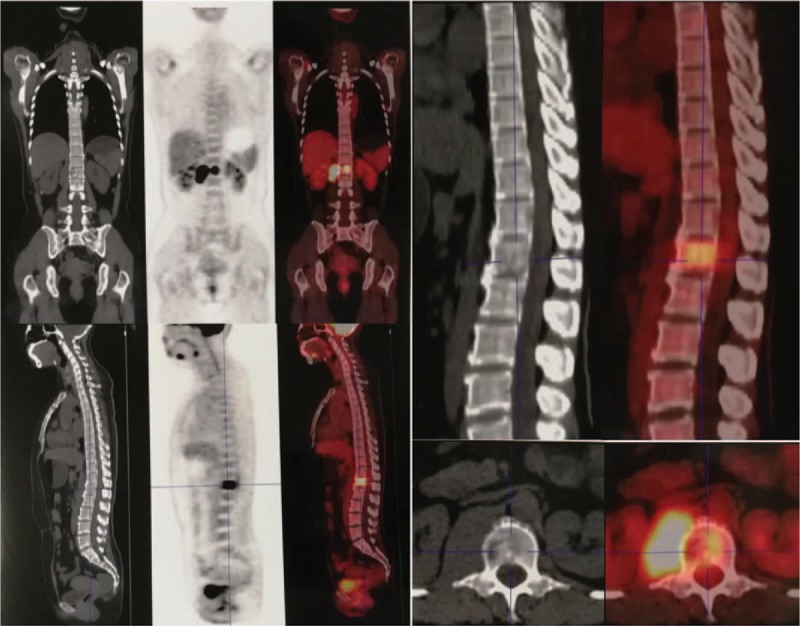
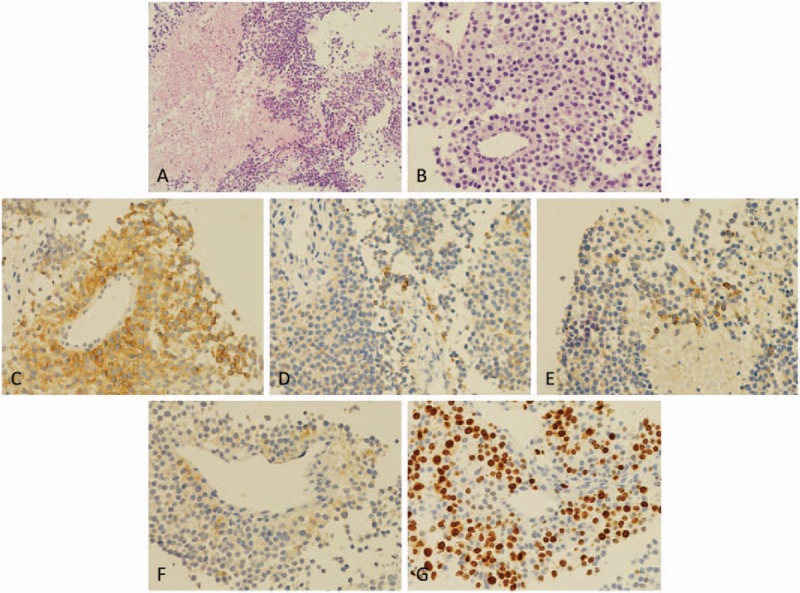
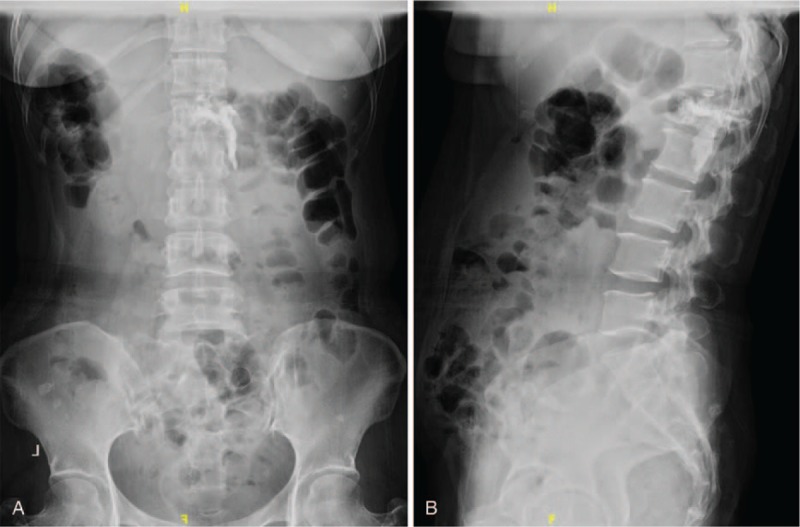
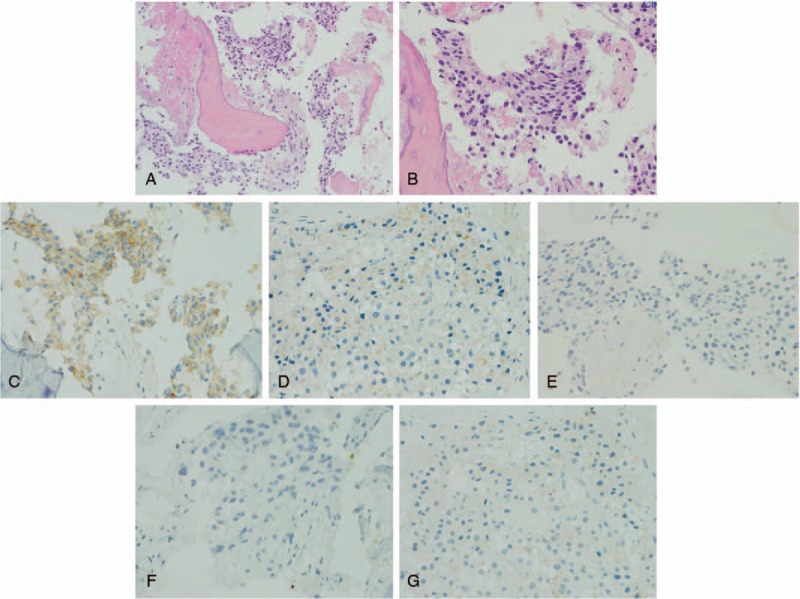
Diagnosis: Magnetic resonance imaging of spine showed vertebral pathological fracture of L1, spinal cord compression secondary to the epidural component of the L1 mass, with increased metastatic marrow infiltration of the right L1 vertebral body, which presented as a solid tumor. Postoperative pathology confirmed the diagnosis of spinal metastases of adrenocortical carcinoma.
Interventions: The patient underwent cement augmentation via a posterior approach, radiotherapy, radiofrequency ablation of psoas major muscle occupying lesions, right chest wall, liver and kidney recess together with adjuvant PD-1 therapy.
Outcomes: The patient's neurological deficits improved significantly after the surgery, and the postoperative period was uneventful at the 6-month and 1-year follow-up visit. There were no complications associated with the operation during the follow-up period.
Lessons: Combined efforts of specialists from orthopedics, urology, interventional radiology, radiotherapy, pathology, endocrinology, and medical oncology led to the successful diagnosis and management of this patient. Metastatic adrenocortical carcinoma of the spine, although rare, should be part of the differential diagnosis when the patient has a history of adrenal carcinoma and presents with back pain, myelopathy, or radiculopathy. We recommend the posterior approach for total excision of the spinal metastatic adrenocortical carcinoma when the tumor has caused neurological deficits. Osteoplasty by cement augmentation, radiotherapy, and targeted PD-1 therapy may also be good choices for treatment.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Surgical management of spinal metastases of thymic carcinoma: A case report and literature review.Medicine (Baltimore). 2019 Jan;98(3):e14198. doi: 10.1097/MD.0000000000014198. Medicine (Baltimore). 2019. PMID: 30653174 Free PMC article. Review.
-
Surgical treatment of chondrosarcoma of the sacrum with cement augmentation: A case report.Medicine (Baltimore). 2019 Dec;98(50):e18413. doi: 10.1097/MD.0000000000018413. Medicine (Baltimore). 2019. PMID: 31852164 Free PMC article.
-
Surgical treatment of metastatic mesenchymal chondrosarcoma to the spine: A case report.Medicine (Baltimore). 2020 Jan;99(5):e18643. doi: 10.1097/MD.0000000000018643. Medicine (Baltimore). 2020. PMID: 32000368 Free PMC article.
-
Surgical treatment of giant chordoma in the thoracic spine combining thoracoscopic and posterior spinal surgery: A case report.Medicine (Baltimore). 2019 Aug;98(35):e16990. doi: 10.1097/MD.0000000000016990. Medicine (Baltimore). 2019. PMID: 31464948 Free PMC article.
-
Successful treatment of malignant thymoma with sacrum metastases: A case report and review of literature.Medicine (Baltimore). 2018 Dec;97(51):e13796. doi: 10.1097/MD.0000000000013796. Medicine (Baltimore). 2018. PMID: 30572538 Free PMC article. Review.
Cited by
-
Uncommon Metastasizing Site of Adrenocortical Carcinoma.Cureus. 2021 May 27;13(5):e15267. doi: 10.7759/cureus.15267. Cureus. 2021. PMID: 34221746 Free PMC article.
-
Thermal ablation in adrenal disorders: a discussion of the technology, the clinical evidence and the future.Curr Opin Endocrinol Diabetes Obes. 2021 Jun 1;28(3):291-302. doi: 10.1097/MED.0000000000000627. Curr Opin Endocrinol Diabetes Obes. 2021. PMID: 33741778 Free PMC article. Review.
References
-
- Kebebew E, Reiff E, Duh QY, et al. Extent of disease at presentation and outcome for adrenocortical carcinoma: have we made progress? World J Surg 2006;30:872–8. - PubMed
-
- Abiven G, Coste J, Groussin L, et al. Clinical and biological features in the prognosis of adrenocortical cancer: poor outcome of cortisol-secreting tumors in a series of 202 consecutive patients. J Clin Endocrinol Metab 2006;91:2650–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
