

Body Composition, Adherence to Anthracycline and Taxane-Based Chemotherapy, and Survival After Nonmetastatic Breast Cancer
- PMID: 31804676
- PMCID: PMC6902178
- DOI: 10.1001/jamaoncol.2019.4668
Body Composition, Adherence to Anthracycline and Taxane-Based Chemotherapy, and Survival After Nonmetastatic Breast Cancer
Abstract
Importance: Although most chemotherapies are dosed on body surface area or weight, body composition (ie, the amount and distribution of muscle and adipose tissues) is thought to be associated with chemotherapy tolerance and adherence.
Objectives: To evaluate whether body composition is associated with relative dose intensity (RDI) on anthracycline and taxane-based chemotherapy or hematologic toxic effects and whether lower RDI mediates the association of adiposity with mortality.
Design, setting, and participants: An observational cohort study with prospectively collected electronic medical record data was conducted at Kaiser Permanente Northern California, a multicenter, community oncology setting within an integrated health care delivery system. Participants included 1395 patients with nonmetastatic breast cancer diagnosed between January 1, 2005, and December 31, 2013, and treated with anthracycline and taxane-based chemotherapy. Data analysis was performed between February 25 and September 4, 2019.
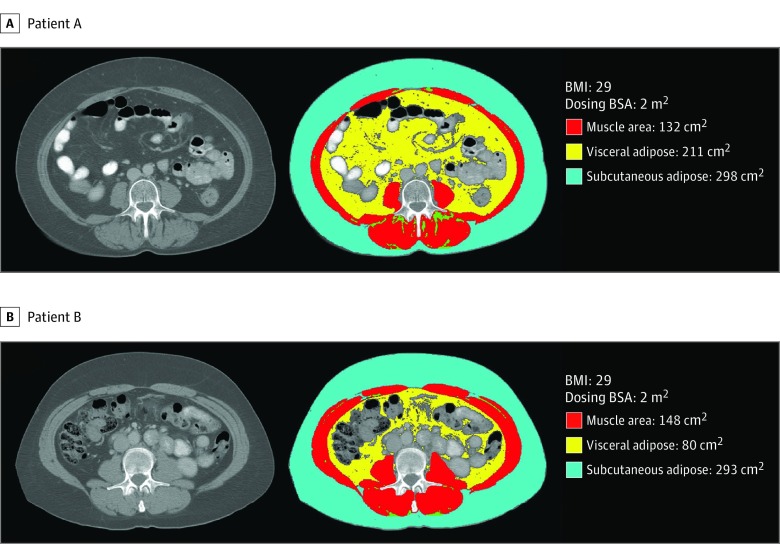
Exposures: Intramuscular, visceral, and subcutaneous adiposity as well as skeletal muscle were evaluated from clinically acquired computed tomographic scans at diagnosis.
Main outcomes and measures: The primary outcome was low RDI (<0.85), which is the ratio of delivered to planned chemotherapy dose, derived from infusion records; in addition, hematologic toxic effects were defined based on laboratory test values. To evaluate associations with overall and breast cancer-specific mortality, logistic regression models adjusted for age and body surface area were fit as well as Cox proportional hazards models adjusted for age, race/ethnicity, adiposity, Charlson comorbidity index score, and tumor stage and subtype. The mediation proportion was computed using the difference method.
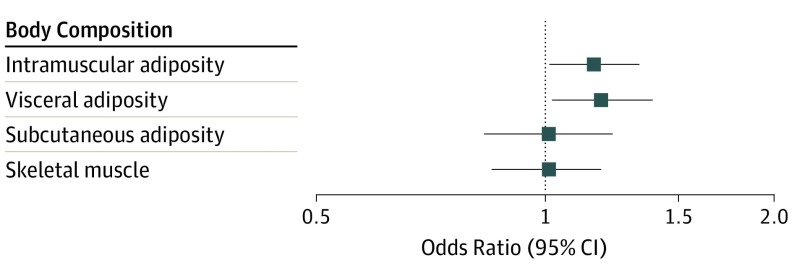
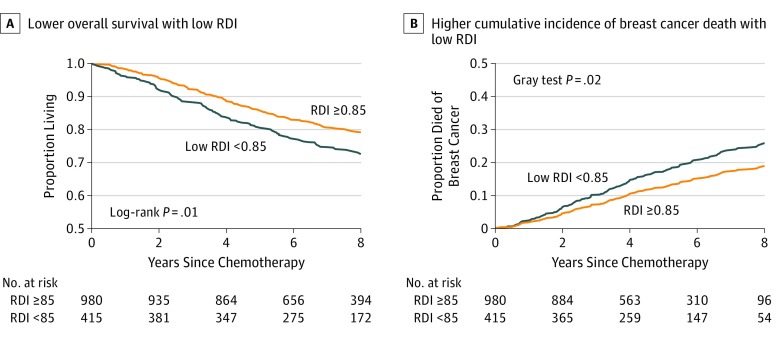
Results: The mean (SD) age at diagnosis of the 1395 women included in the study was 52.8 (10.2) years. Greater visceral (odds ratio [OR], 1.19; 95% CI, 1.02-1.39 per SD) and intramuscular (OR, 1.16; 95% CI, 1.01-1.34 per SD) adiposity were associated with increased odds of RDI less than 0.85. Greater muscle mass was associated with a decreased odds of hematologic toxic effects (OR, 0.84; 95% CI, 0.71-0.98 per SD). Relative dose intensity less than 0.85 was associated with a 30% increased risk of death (hazard ratio, 1.30; 95% CI, 1.02-1.65). Lower RDI partially explained the association of adiposity with breast cancer-specific mortality (mediation proportion, 0.20; 95% CI, 0.05-0.55).
Conclusions and relevance: Excess adiposity, presenting as larger visceral or intramuscular adiposity, was associated with lower RDI. Lower RDI partially mediated the association of adiposity with worse breast cancer-specific survival. Body composition may help to identify patients likely to experience toxic effects and subsequent dose delays or reductions, which could compromise chemotherapeutic efficacy.
Conflict of interest statement
Figures
References
-
- National Cancer Institute Surveillance Epidemiology and End Results Cancer stat facts: female breast cancer. Cancer Statistics 2015; https://seer.cancer.gov/statfacts/html/breast.html. Accessed September 19, 2018.
-
- Muss HB, Berry DA, Cirrincione C, et al. ; Cancer and Leukemia Group B Experience . Toxicity of older and younger patients treated with adjuvant chemotherapy for node-positive breast cancer: the Cancer and Leukemia Group B Experience. J Clin Oncol. 2007;25(24):3699-3704. doi:10.1200/JCO.2007.10.9710 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
