

In vivo ultrasound thermal ablation control using echo decorrelation imaging in rabbit liver and VX2 tumor
- PMID: 31805129
- PMCID: PMC6894854
- DOI: 10.1371/journal.pone.0226001
In vivo ultrasound thermal ablation control using echo decorrelation imaging in rabbit liver and VX2 tumor
Abstract
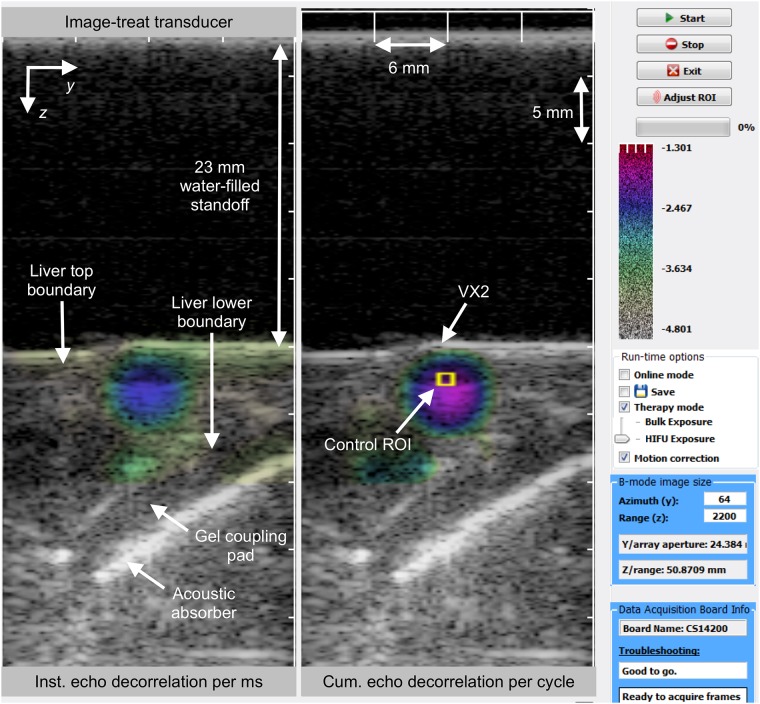
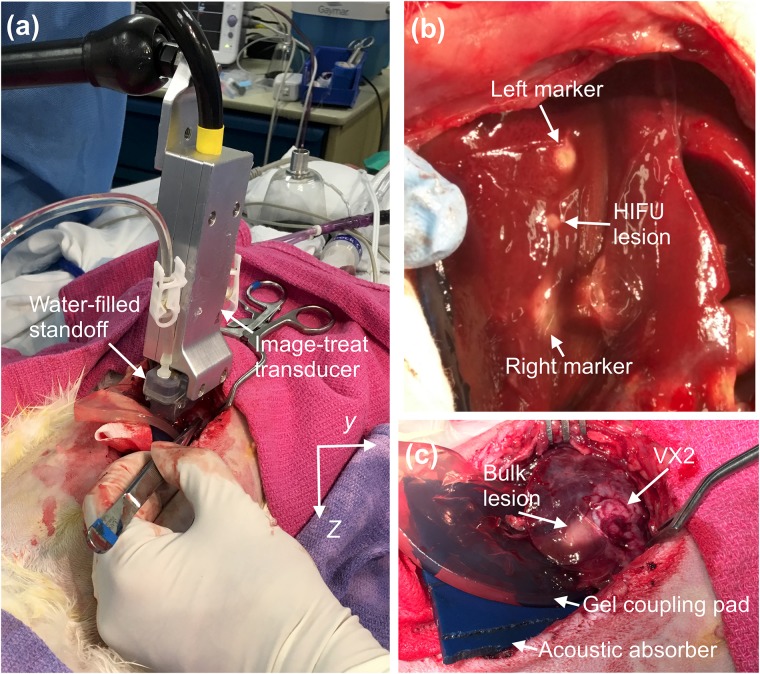
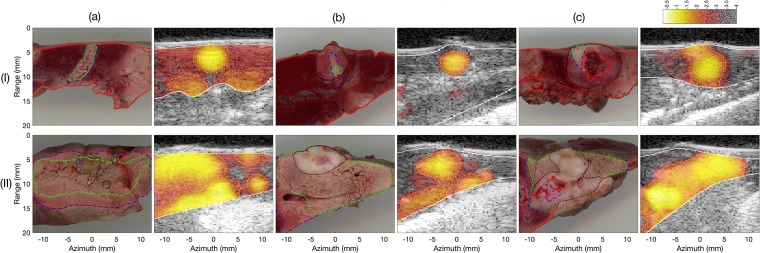
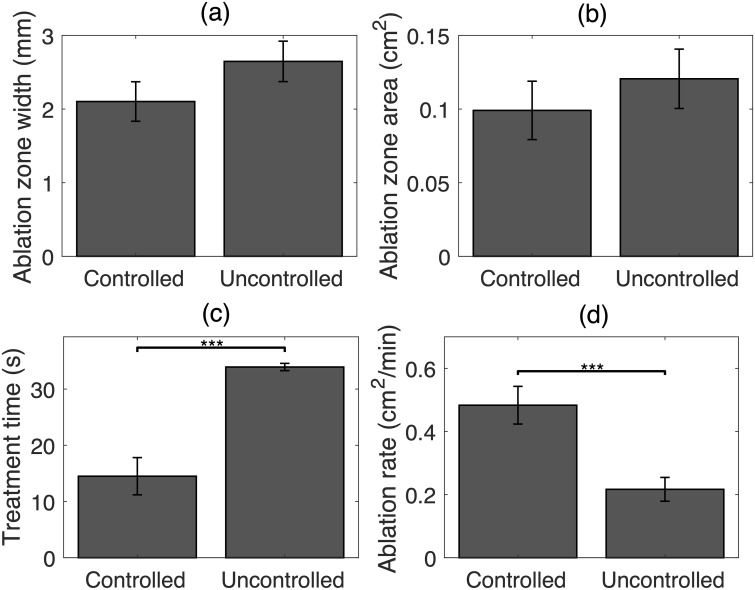
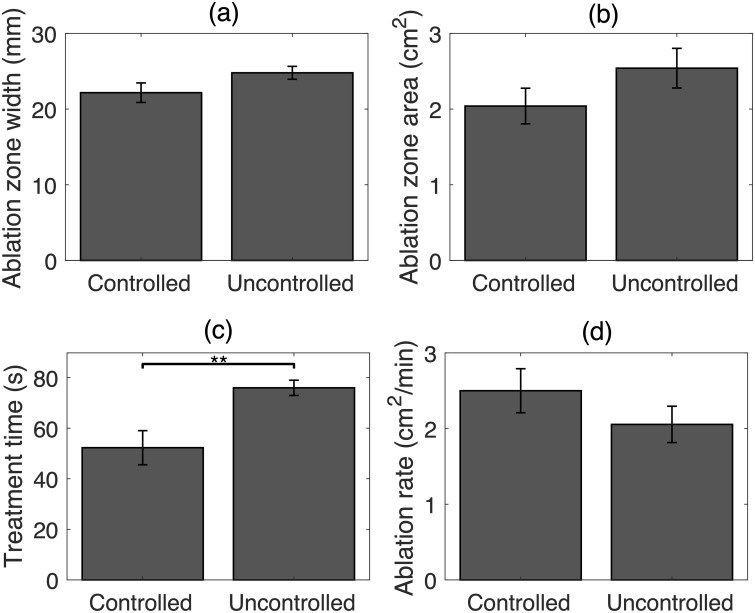
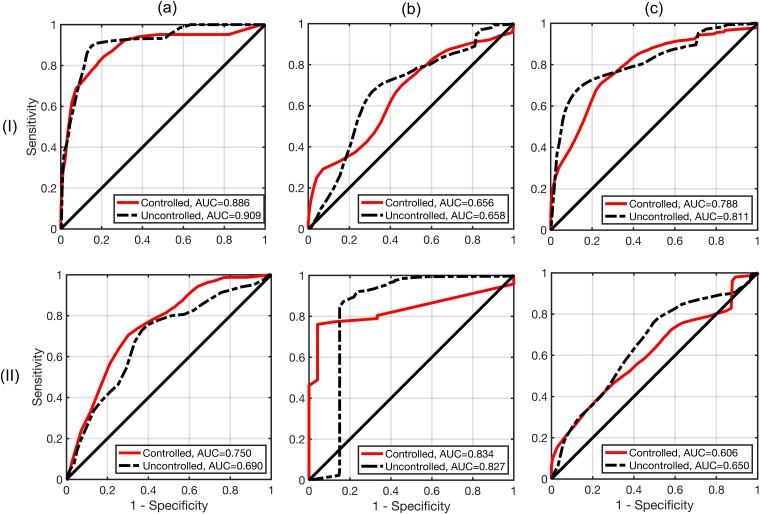
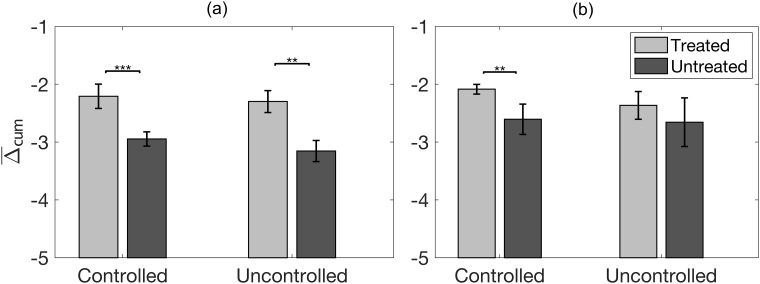
The utility of echo decorrelation imaging feedback for real-time control of in vivo ultrasound thermal ablation was assessed in rabbit liver with VX2 tumor. High-intensity focused ultrasound (HIFU) and unfocused (bulk) ablation were performed using 5 MHz linear image-ablate arrays. Treatments comprised up to nine lower-power sonications, followed by up to nine higher-power sonications, ceasing when the average cumulative echo decorrelation within a control region of interest exceeded a predefined threshold (- 2.3, log10-scaled echo decorrelation per millisecond, corresponding to 90% specificity for tumor ablation prediction in previous in vivo experiments). This threshold was exceeded in all cases for both HIFU (N = 12) and bulk (N = 8) ablation. Controlled HIFU trials achieved a significantly higher average ablation rate compared to comparable ablation trials without image-based control, reported previously. Both controlled HIFU and bulk ablation trials required significantly less treatment time than these previous uncontrolled trials. Prediction of local liver and VX2 tumor ablation using echo decorrelation was tested using receiver operator characteristic curve analysis, showing prediction capability statistically equivalent to uncontrolled trials. Compared to uncontrolled trials, controlled trials resulted in smaller thermal ablation regions and higher contrast between echo decorrelation in treated vs. untreated regions. These results indicate that control using echo decorrelation imaging may reduce treatment duration and increase treatment reliability for in vivo thermal ablation.
Conflict of interest statement
One author (PGB) was employed by Guided Therapy Systems/Ardent Sound, a company that develops and markets therapeutic ultrasound products. The research materials provided for this study are prototypes incorporating technology patented by Guided Therapy Systems/Ardent Sound, but do not comprise a commercial product, either marketed or under development. This affiliation does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
