

A randomized controlled trial on analgesic effect of repeated Quadratus Lumborum block versus continuous epidural analgesia following laparoscopic nephrectomy
- PMID: 31805855
- PMCID: PMC6894195
- DOI: 10.1186/s12871-019-0891-7
A randomized controlled trial on analgesic effect of repeated Quadratus Lumborum block versus continuous epidural analgesia following laparoscopic nephrectomy
Abstract
Background: Epidural analgesia as the effective pain management for abdominal surgery has side effects such as paresthesia, hypotension, hematomas, and impaired motoric of lower limbs. The quadratus lumborum block (QLB) has potential as an abdominal truncal block, however, its analgesic efficacy has never been compared to epidural analgesia on laparoscopic nephrectomy. This prospective randomized controlled study compared the effectiveness of QLB with the epidural analgesia technique in relieving postoperative pain following transperitoneal laparoscopic nephrectomy.
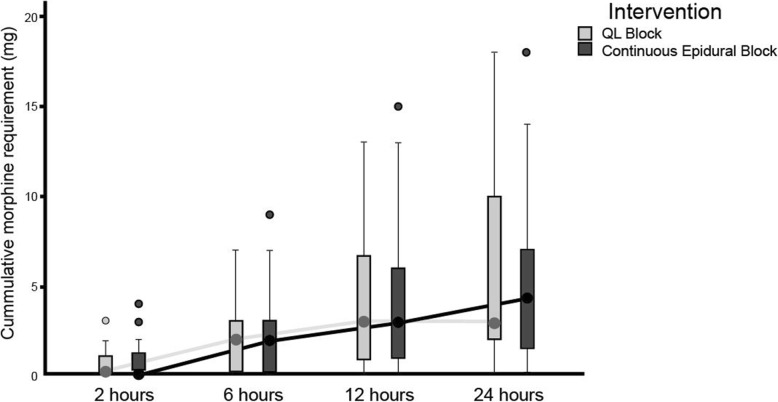
Methods: Sixty-two patients underwent laparoscopic donor nephrectomy and were randomized to receive QLB (n = 31) or continuous epidural (n = 31). The QLB group received bilateral QLB using 0.25% bupivacaine and the epidural group received 6 ml/h of 0.25% bupivacaine for intraoperative analgesia. As postoperative analgesia, the QLB group received repeated bilateral QLB with the same dose and the epidural group received 6 ml/h of 0.125% bupivacaine for 24 h after surgery completion. The primary outcome was the 24-h cumulative morphine requirement after surgery. The secondary outcome was the postoperative pain scores. Sensory block coverage, hemodynamic changes, Bromage score, postoperative nausea-vomiting (PONV), paresthesia, and duration of urinary catheter usage were recorded and analyzed.
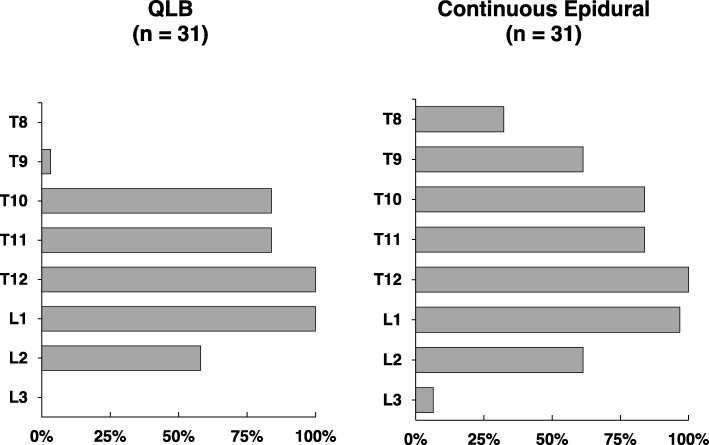
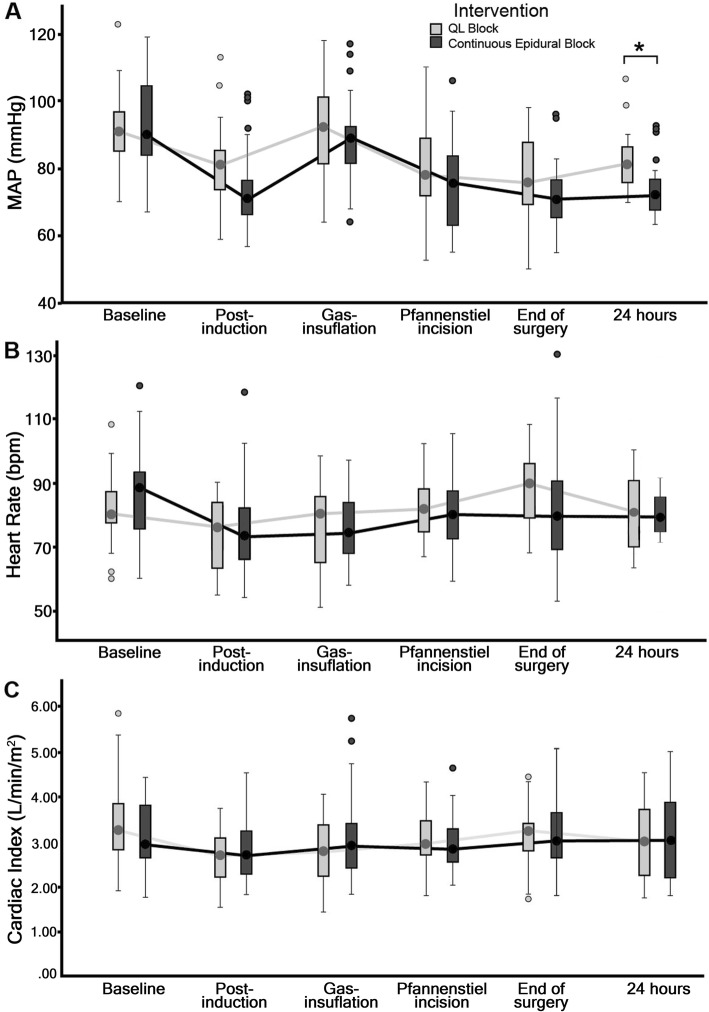
Result: The 24-h cumulative morphine requirement and pain scores after surgery were comparable between the QLB and epidural groups. The coverage of QLB was extended from T9 to L2 and the continuous epidural block was extended from T8 to L3 dermatomes. The mean arterial pressure (MAP) measured at 24 h after surgery was lower in the epidural group (p = 0.001). Bromage score, incidence of PONV, and paresthesia were not significantly different between the two groups. Duration of urinary catheter usage was shorter (p < 0.001) in the QLB group.
Conclusion: The repeated QLB had a similar 24-h cumulative morphine requirement, comparable postoperative pain scores and sensory blockade, higher postoperative MAP, a similar degree of motoric block, no difference in the incidence of PONV and paresthesia, and shorter urinary catheter usage, compared to the continuous epidural analgesia following transperitoneal laparoscopic nephrectomy.
Trial registration: ClinicalTrial.gov NCT03520205 retrospectively registered on May 9th 2018.
Keywords: Epidural analgesia; Laparoscopic nephrectomy; Patient-controlled analgesia; Postoperative analgesia; Quadratus lumborum block.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Wibisono Elita, Mochtar Chaidir Arif, Hamid Agus Rizal A. H, Widia Fina, Sukmono R. Besthadi, Wahyudi Irfan. Laparoscopic Living Donor Nephrectomy in Cipto Mangunkusumo Hospital: Postoperative Pain and Recovery Analysis. Advanced Science Letters. 2018;24(9):6704–6708. doi: 10.1166/asl.2018.12816. - DOI
-
- Sahajananda H. Jyothi, Punithavathy. Renal transplantation with and without epidural analgesia. Indian J Anesth. 2006;50(3):187–192.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
