

Value-based healthcare in ischemic stroke care: case-mix adjustment models for clinical and patient-reported outcomes
- PMID: 31805876
- PMCID: PMC6896707
- DOI: 10.1186/s12874-019-0864-z
Value-based healthcare in ischemic stroke care: case-mix adjustment models for clinical and patient-reported outcomes
Abstract
Background: Patient-Reported Outcome Measures (PROMs) have been proposed for benchmarking health care quality across hospitals, which requires extensive case-mix adjustment. The current study's aim was to develop and compare case-mix models for mortality, a functional outcome, and a patient-reported outcome measure (PROM) in ischemic stroke care.
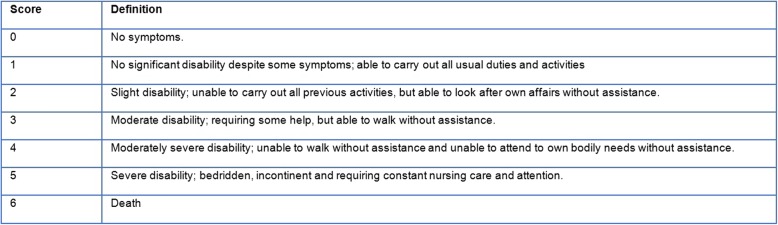
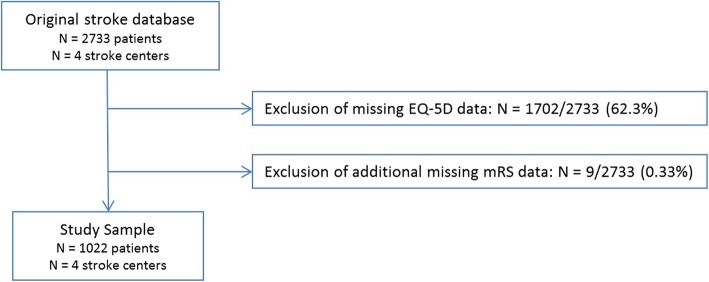
Methods: Data from ischemic stroke patients, admitted to four stroke centers in the Netherlands between 2014 and 2016 with available outcome information (N = 1022), was analyzed. Case-mix adjustment models were developed for mortality, modified Rankin Scale (mRS) scores and EQ-5D index scores with respectively binary logistic, proportional odds and linear regression models with stepwise backward selection. Predictive ability of these models was determined with R-squared (R2) and area-under-the-receiver-operating-characteristic-curve (AUC) statistics.
Results: Age, NIHSS score on admission, and heart failure were the only common predictors across all three case-mix adjustment models. Specific predictors for the EQ-5D index score were sex (β = 0.041), socio-economic status (β = - 0.019) and nationality (β = - 0.074). R2-values for the regression models for mortality (5 predictors), mRS score (9 predictors) and EQ-5D utility score (12 predictors), were respectively R2 = 0.44, R2 = 0.42 and R2 = 0.37.
Conclusions: The set of case-mix adjustment variables for the EQ-5D at three months differed considerably from the set for clinical outcomes in stroke care. The case-mix adjustment variables that were specific to this PROM were sex, socio-economic status and nationality. These variables should be considered in future attempts to risk-adjust for PROMs during benchmarking of hospitals.
Keywords: Case-mix; Ischemic stroke; Patient-reported outcome measure; Risk adjustment model; Value-based healthcare.
Conflict of interest statement
- Authors AO and JH are supported by a grant from the Federation of Dutch University Medical Centers (NFU).
- Author DD reports grants and other from Stryker European Operations BV, grants from Penumbra Inc., grants from Medtronic, grants from Dutch Heart Foundation, grants from Brain Foundation Netherlands, grants from ZON MW () and grants from Thrombolytic Science, LLC, outside the submitted work.
- Remaining authors declare no competing interests.
- This study was a cooperation of 8 parties: Stroke Knowledge Network Netherlands, Achmea Holding N.V., Netherlands Federation of University Medical Centres (NFU), Dutch Association for Neurology (NVN), Netherlands Society of Rehabilitation Medicine (VRA), Dutch Association of Elderly Care Physicians and Social Geriatricians (Verenso), The Dutch College of General Practitioners (NHG), Dutch Institute for Clinical Auditing (DICA), National Health Care Institute (ZN).
Figures

References
-
- Katzan IL, Spertus J, Bettger JP, Bravata DM, Reeves MJ, Smith EE, et al. Risk adjustment of ischemic stroke outcomes for comparing hospital performance: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(3):918–944. doi: 10.1161/01.str.0000441948.35804.77. - DOI - PubMed
-
- Kotronoulas G, Kearney N, Maguire R, Harrow A, Di Domenico D, Croy S, et al. What is the value of the routine use of patient-reported outcome measures toward improvement of patient outcomes, processes of care, and health service outcomes in cancer care? A systematic review of controlled trials. J Clin Oncol. 2014;32(14):1480–1501. doi: 10.1200/JCO.2013.53.5948. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
