

The coin model of privilege and critical allyship: implications for health
- PMID: 31805907
- PMCID: PMC6896777
- DOI: 10.1186/s12889-019-7884-9
The coin model of privilege and critical allyship: implications for health
Abstract
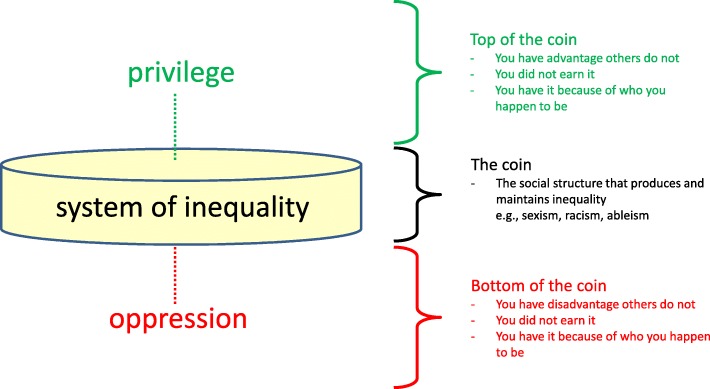
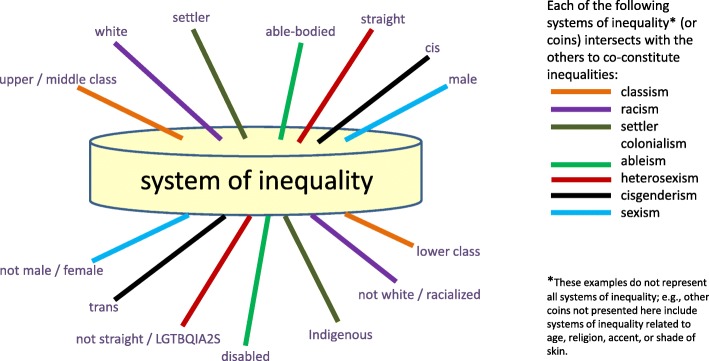
Health inequities are widespread and persistent, and the root causes are social, political and economic as opposed to exclusively behavioural or genetic. A barrier to transformative change is the tendency to frame these inequities as unfair consequences of social structures that result in disadvantage, without also considering how these same structures give unearned advantage, or privilege, to others. Eclipsing privilege in discussions of health equity is a crucial shortcoming, because how one frames the problem sets the range of possible solutions that will follow. If inequity is framed exclusively as a problem facing people who are disadvantaged, then responses will only ever target the needs of these groups without redressing the social structures causing disadvantages. Furthermore, responses will ignore the complicity of the corollary groups who receive unearned and unfair advantage from these same structures. In other words, we are missing the bigger picture. In this conceptualization of health inequity, we have limited the potential for disruptive action to end these enduring patterns.The goal of this article is to advance understanding and action on health inequities and the social determinants of health by introducing a framework for transformative change: the Coin Model of Privilege and Critical Allyship. First, I introduce the model, which explains how social structures produce both unearned advantage and disadvantage. The model embraces an intersectional approach to understand how systems of inequality, such as sexism, racism and ableism, interact with each other to produce complex patterns of privilege and oppression. Second, I describe principles for practicing critical allyship to guide the actions of people in positions of privilege for resisting the unjust structures that produce health inequities. The article is a call to action for all working in health to (1) recognize their positions of privilege, and (2) use this understanding to reorient their approach from saving unfortunate people to working in solidarity and collective action on systems of inequality.
Keywords: Ableism; Allyship; Health equity; Indigenous health; Intersectionality; Oppression; Privilege; Racism; Social determinants of health; Social justice.
Conflict of interest statement
I have no conflicts of interest to declare.
Figures
References
-
- Simons D. The Monkey Business Illusion. https://www.youtube.com/watch?v=IGQmdoK_ZfY. Accessed 28 July 2019.
-
- Nixon SA. What every health researcher needs to know about health equity: privilege, Oppression and Allyship University of Manitoba Dec 1, 2017. https://www.youtube.com/watch?time_continue=1561&v=APdNxzsqnz4. Accessed 28 July 2019.
-
- World Health Organization Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Final Report. Geneva: WHO; 2008. http://www.who.int/social_determinants/thecommission/finalreport/en/. Accessed 28 July 2019.
-
- Dhillon J. Prairie rising: indigenous youth, decolonization, and the politics of intervention. Toronto: University of Toronto Press; 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
