

Association Between Patient Cost Sharing and Cardiac Rehabilitation Adherence
- PMID: 31806097
- PMCID: PMC6946372
- DOI: 10.1016/j.mayocp.2019.07.018
Association Between Patient Cost Sharing and Cardiac Rehabilitation Adherence
Abstract
Objective: To determine the association between cost sharing and adherence to cardiac rehabilitation (CR).
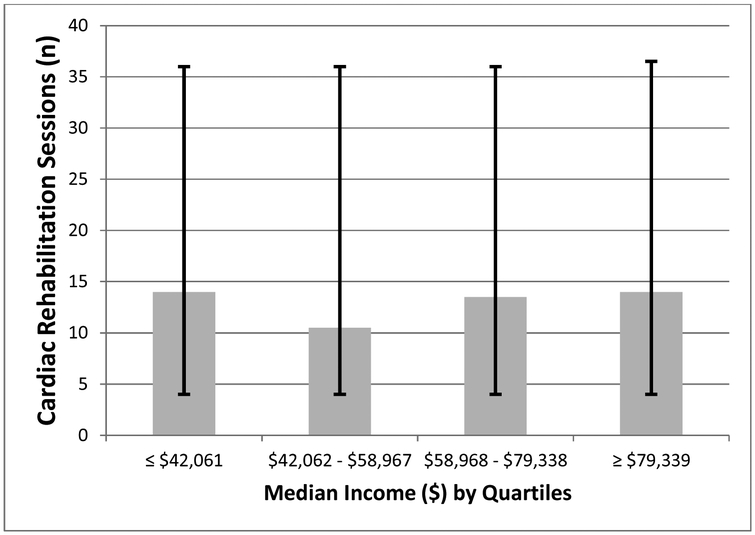
Patients and methods: We collected detailed cost-sharing information for patients enrolled in CR at Baystate Medical Center in Springfield, Massachusetts, including the presence (or absence) and amounts of co-pays and deductibles. We evaluated the association between cost sharing and the total number of CR sessions attended as well as the influence of household income on CR attendance.
Results: In 2015, 603 patients enrolled in CR had complete cost-sharing information. In total, 235 (39%) had some form of cost sharing. Of these, 192 (82%) had co-pays (median co-pay, $20; interquartile range [IQR], $10-$32) and 79 (34%) had an unmet deductible (median, $500; IQR, $250-$1800). The presence of any amount or form of cost sharing was associated with 6 fewer sessions of CR (16; IQR, 4-36 vs 10; IQR, 4-27; P<.001). Patients hospitalized in November or December with deductibles that renewed in January attended 4.5 fewer sessions of CR (8.5; IQR, 3.25-12.50 vs 13; IQR, 5.25-36.00; P=.049). After adjustment for differences in baseline characteristics, every $10 increase in co-pay was associated with 1.5 (95% CI, -2.3 to -0.7) fewer sessions of CR (P<.001). Household income did not moderate these relationships.
Conclusion: Cost sharing was associated with lower CR attendance and exhibited a dose-response relationship such that higher cost sharing was associated with lower CR attendance. Given that CR is cost-effective and underutilized, insurance companies and other payers should reevaluate their cost-sharing policies for CR.
Copyright © 2019 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Cost-Sharing Deters Cardiac Rehabilitation Adherence.Mayo Clin Proc. 2019 Dec;94(12):2372-2374. doi: 10.1016/j.mayocp.2019.10.019. Mayo Clin Proc. 2019. PMID: 31806091 No abstract available.
References
-
- Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med. 2005;143(9):659–672. - PubMed
-
- Piepoli MF, Davos C, Francis DP, Coats AJS, ExTraMATCH Collaborative. Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ. 2004;328(7433):189. doi:10.1136/bmj.37938.645220.EE - DOI - PMC - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106 - DOI - PMC - PubMed
-
- Members WC, Thomas RJ, Balady G, et al. 2018 ACC/AHA Clinical Performance and Quality Measures for Cardiac Rehabilitation: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Journal of the American College of Cardiology. March 2018:24587. doi:10.1016/j.jacc.2018.01.004 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
