

Within-Trial Evaluation of Medical Resources, Costs, and Quality of Life Among Patients With Type 2 Diabetes Participating in the Exenatide Study of Cardiovascular Event Lowering (EXSCEL)
- PMID: 31806653
- PMCID: PMC7210004
- DOI: 10.2337/dc19-0950
Within-Trial Evaluation of Medical Resources, Costs, and Quality of Life Among Patients With Type 2 Diabetes Participating in the Exenatide Study of Cardiovascular Event Lowering (EXSCEL)
Abstract
Objective: To compare medical resource use, costs, and health utilities for 14,752 patients with type 2 diabetes who were randomized to once-weekly exenatide (EQW) or placebo in addition to usual diabetes care in the Exenatide Study of Cardiovascular Event Lowering (EXSCEL).
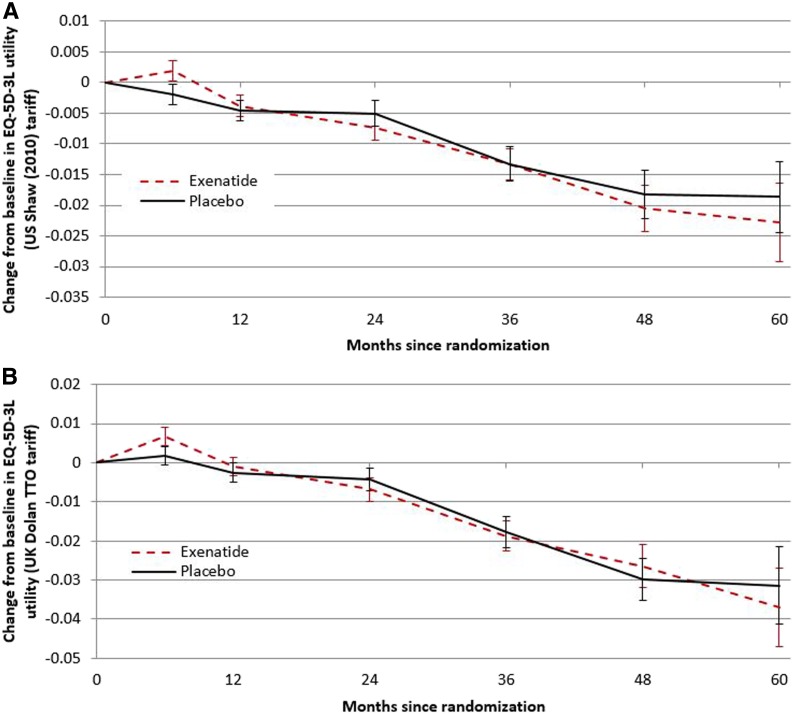
Research design and methods: Medical resource use data and responses to the EuroQol 5-Dimension (EQ-5D) instrument were collected at baseline and throughout the trial. Medical resources and medications were assigned values by using U.S. Medicare payments and wholesale acquisition costs, respectively. Secondary analyses used English costs.
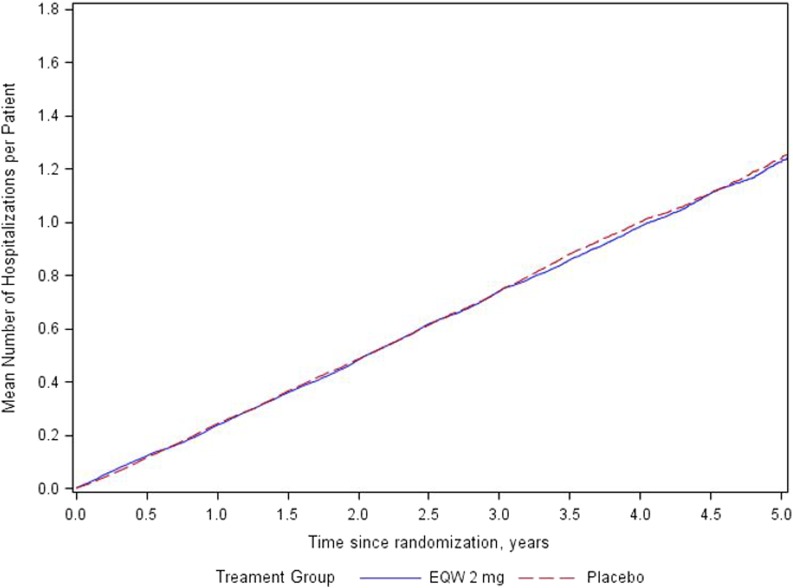
Results: Patients were followed for an average of 3.3 years, during which time those randomized to EQW experienced 0.41 fewer inpatient days (7.05 vs. 7.46 days; relative rate ratio 0.91; P = 0.05). Rates of outpatient medical visits were similar, as were total inpatient and outpatient costs. Mean costs for nonstudy diabetes medications over the study period were ∼$1,600 lower with EQW than with placebo (P = 0.01). Total within-study costs, excluding study medication, were lower in the EQW arm than in the placebo arm ($28,907 vs. $30,914; P ≤ 0.01). When including the estimated cost of EQW, total mean costs were significantly higher in the EQW group than in the placebo group ($42,697 vs. $30,914; P < 0.01). With English costs applied, mean total costs, including exenatide costs, were £1,670 higher in the EQW group than the placebo group (£10,874 vs. £9,204; P < 0.01). There were no significant differences in EQ-5D health utilities between arms over time.
Conclusions: Medical costs were lower in the EQW arm than the placebo arm, but total costs were significantly higher once the cost of branded exenatide was incorporated.
Trial registration: ClinicalTrials.gov NCT01144338.
© 2019 by the American Diabetes Association.
Figures
References
-
- Cho NH, Shaw JE, Karuranga S, et al. . IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 2018;138:271–281 - PubMed
-
- Sarwar N, Gao P, Seshasai SR, et al. .; Emerging Risk Factors Collaboration . Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies [published correction appears in Lancet 2010;376:958]. Lancet 2010;375:2215–2222 - PMC - PubMed
-
- Tancredi M, Rosengren A, Svensson A-M, et al. . Excess mortality among persons with type 2 diabetes. N Engl J Med 2015;373:1720–1732 - PubMed
-
- Holman RR, Bethel MA, George J, et al. . Rationale and design of the EXenatide Study of Cardiovascular Event Lowering (EXSCEL) trial. Am Heart J 2016;174:103–110 - PubMed
