

Brain immunology and immunotherapy in brain tumours
- PMID: 31806885
- PMCID: PMC7327710
- DOI: 10.1038/s41568-019-0224-7
Brain immunology and immunotherapy in brain tumours
Abstract
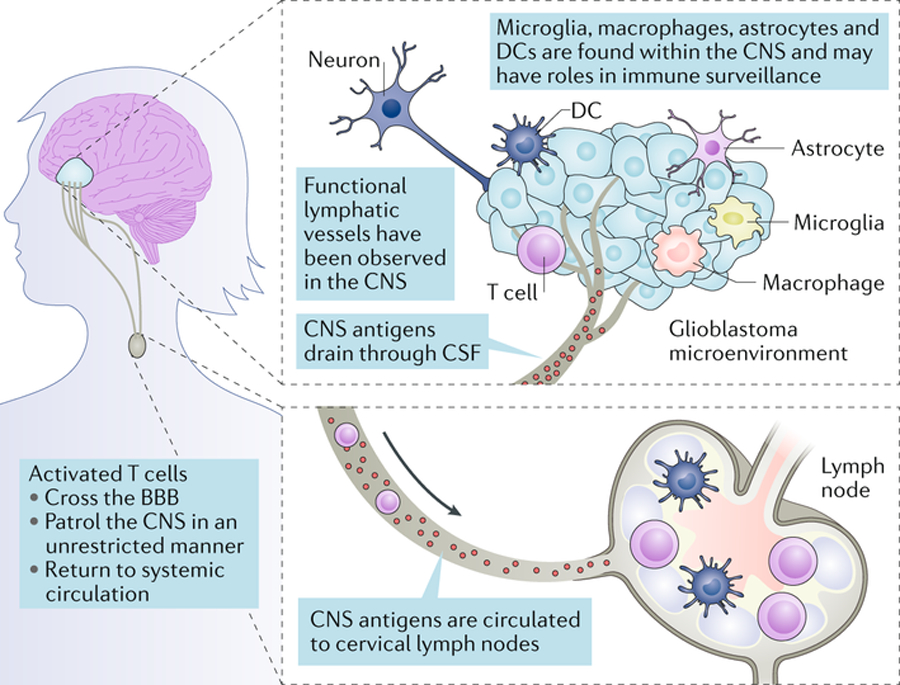
Gliomas, the most common malignant primary brain tumours, remain universally lethal. Yet, seminal discoveries in the past 5 years have clarified the anatomy, genetics and function of the immune system within the central nervous system (CNS) and altered the paradigm for successful immunotherapy. The impact of standard therapies on the response to immunotherapy is now better understood, as well. This new knowledge has implications for a broad range of tumours that develop within the CNS. Nevertheless, the requirements for successful therapy remain effective delivery and target specificity, while the dramatic heterogeneity of malignant gliomas at the genetic and immunological levels remains a profound challenge.
Conflict of interest statement
Figures
References
-
- Stupp R et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med 352, 987–996 (2005). - PubMed
-
- Stummer W et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol 7, 392–401 (2006). - PubMed
-
- Walker MD et al. Randomized comparisons of radiotherapy and nitrosoureas for the treatment of malignant glioma after surgery. N. Engl. J. Med 303, 1323–1329 (1980). - PubMed
-
- Hegi ME et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N. Engl. J. Med 352, 997–1003 (2005). - PubMed
-
- Imperato JP, Paleologos NA & Vick NA Effects of treatment on long-term survivors with malignant astrocytomas. Ann. Neurol 28, 818–822 (1990). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
