

Effect of glucocorticoids on mortality in patients with acute respiratory distress syndrome: A meta-analysis
- PMID: 31807156
- PMCID: PMC6878883
- DOI: 10.3892/etm.2019.8156
Effect of glucocorticoids on mortality in patients with acute respiratory distress syndrome: A meta-analysis
Abstract
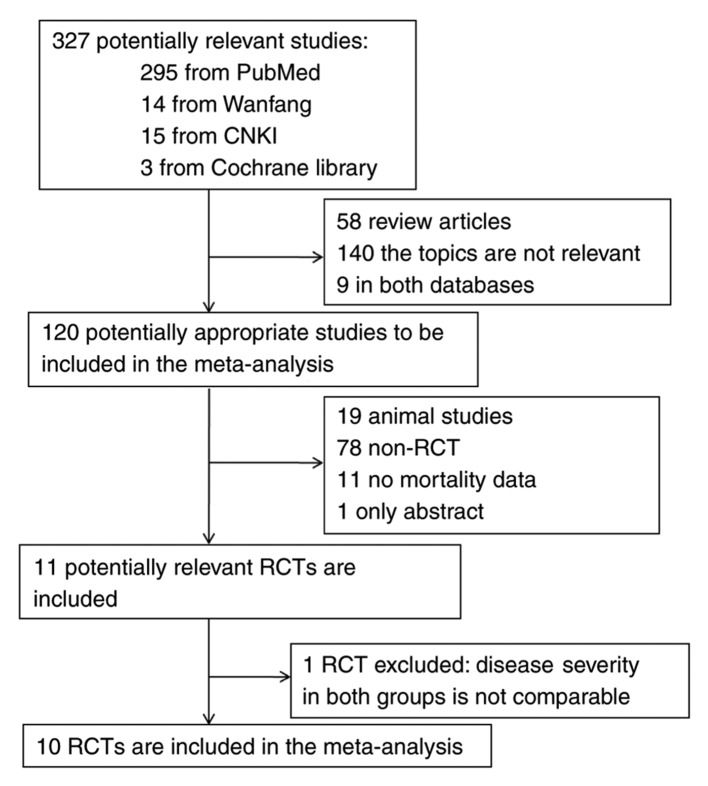
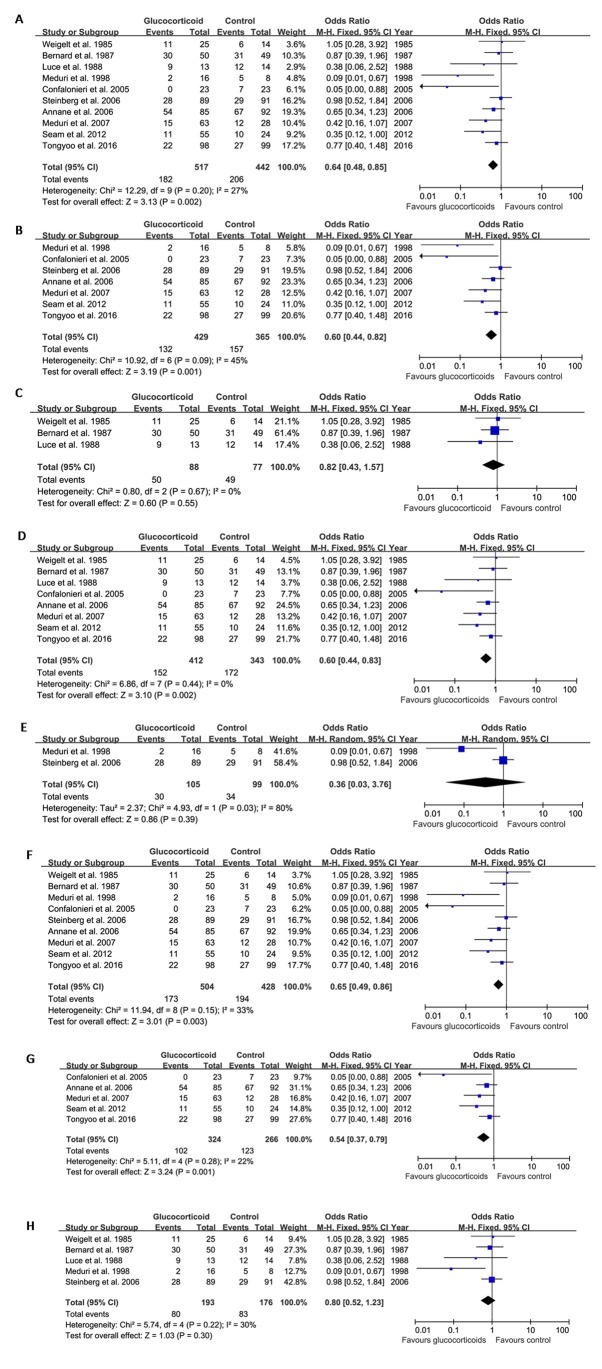
To date, the efficacy of glucocorticoid therapy to reduce mortality in patients with acute respiratory distress syndrome (ARDS) has remained controversial among the studies available. The present meta-analysis study aimed to further clarify the impact of glucocorticoid therapy on mortality in patients with ARDS by performing a pooled analysis of the previous data. The PubMed, Chinese Knowledge Infrastructure, Wanfang and Cochrane trials databases were searched for relevant studies published between 1966 and 2016. Randomized controlled trials (RCTs) that included the use of glucocorticoids in patients with ARDS and had reported on mortality were included. Odds ratios (OR) and 95% confidence intervals (CI) for mortality were calculated. A total of 10 RCTs were included in the meta-analysis. Of these, 4 studies used high-dose glucocorticoid therapy, while 6 used low-dose glucocorticoid therapy. In the pooled analysis, glucocorticoids were indicated to significantly reduce ARDS-associated mortality (OR=0.64, 95% CI: 0.48-0.85, P=0.002). Further subgroup analysis indicated the following: i) Long-term low-dose glucocorticoid therapy reduced ARDS-associated mortality compared with that in the control group (OR=0.60, 95% CI: 0.44-0.82, P=0.001), whereas high-dose short-term glucocorticoid therapy did not reduce mortality (OR=0.82, 95% CI: 0.43-1.57, P=0.55). ii) Early initiation of glucocorticoid therapy was associated with reduced mortality compared with that in the control group (OR=0.60, 95% CI: 0.44-0.83, P=0.002); however, late initiation did not reduce mortality (OR=0.36, 95% CI: 0.03-3.76, P=0.39). iii) Therapeutic rather than preventive use of glucocorticoids reduced mortality (OR=0.65, 95% CI: 0.49-0.86, P=0.003). Overall, the present meta-analysis suggests that early initiation of long-term low-dose glucocorticoid therapy reduces mortality of patients with ARDS.
Keywords: acute lung injury; acute respiratory distress syndrome; glucocorticoids; mortality.
Copyright © 2019, Spandidos Publications.
Figures
References
-
- Leaver SK, Evans TW. Acute respiratory distress syndrome. BMJ. 2007;335:389–394. doi: 10.1136/bmj.39293.624699.AD. - DOI - PMC - PubMed
-
- Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
LinkOut - more resources
Full Text Sources