

Survival and analysis of prognostic factors for hepatoblastoma: based on SEER database
- PMID: 31807536
- PMCID: PMC6861810
- DOI: 10.21037/atm.2019.09.76
Survival and analysis of prognostic factors for hepatoblastoma: based on SEER database
Abstract
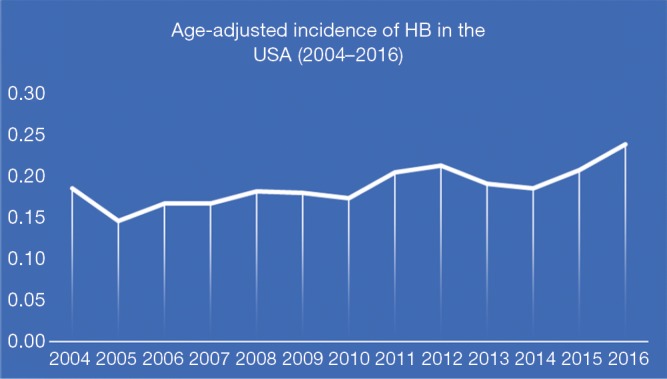
Background: The goal of this study is to assess the newest survival of hepatoblastoma (HB) and the risk factors which impacted on survival by using the Surveillance, Epidemiology and End Results (SEER) database, also calculate the incidence of HB in recent years.
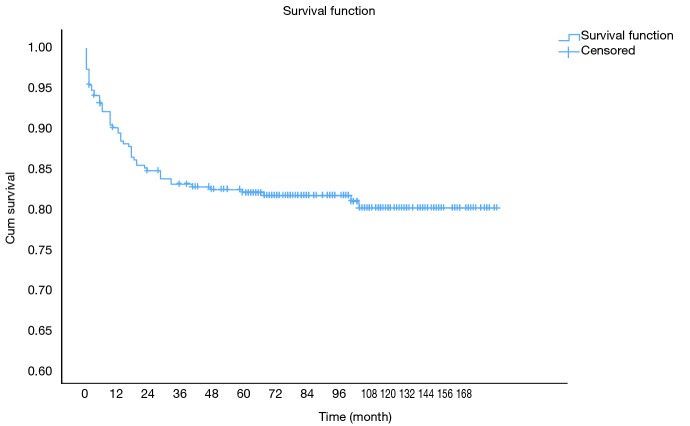
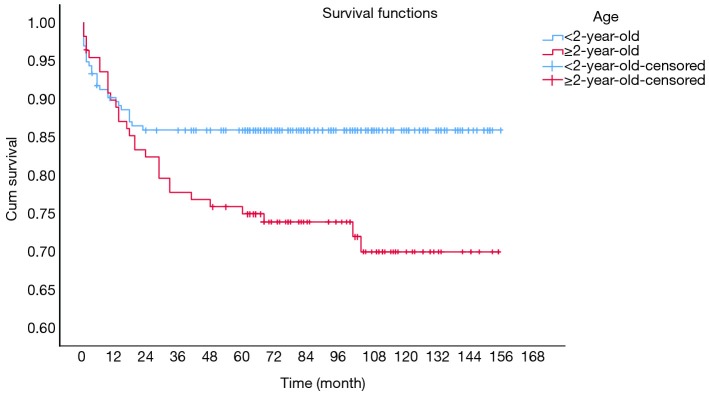
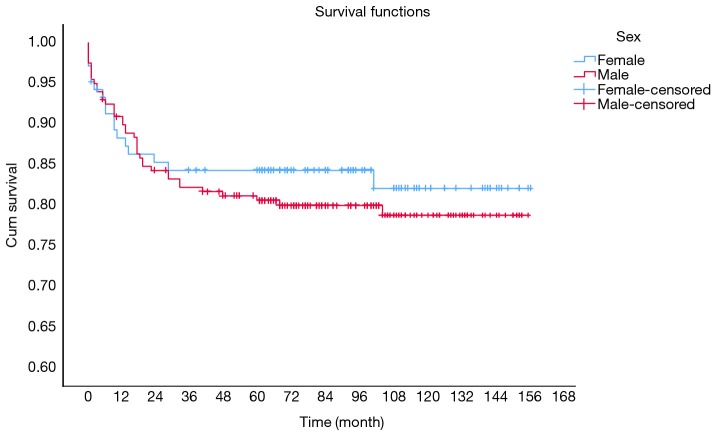
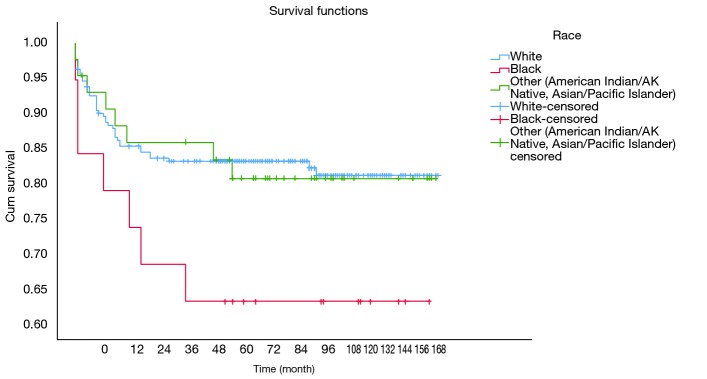
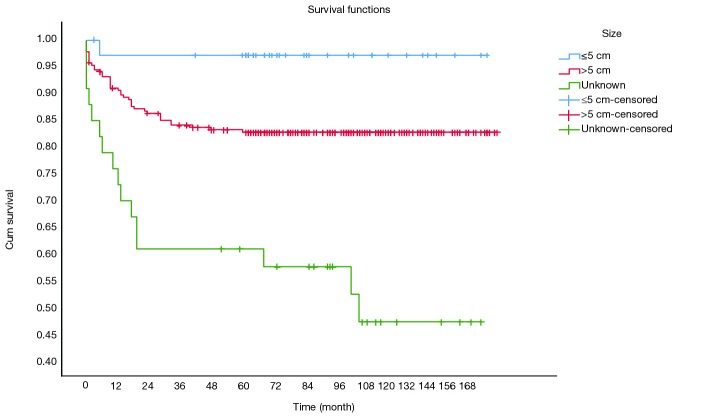
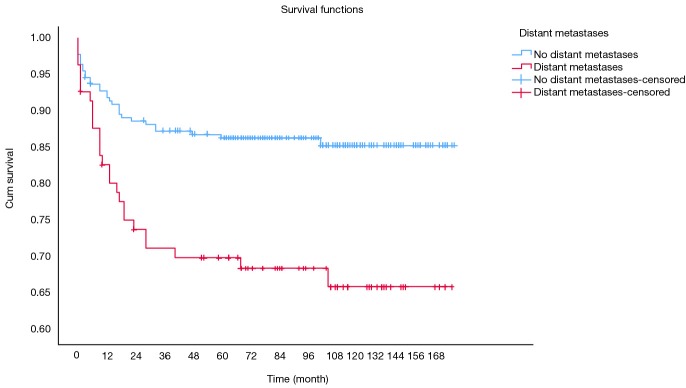
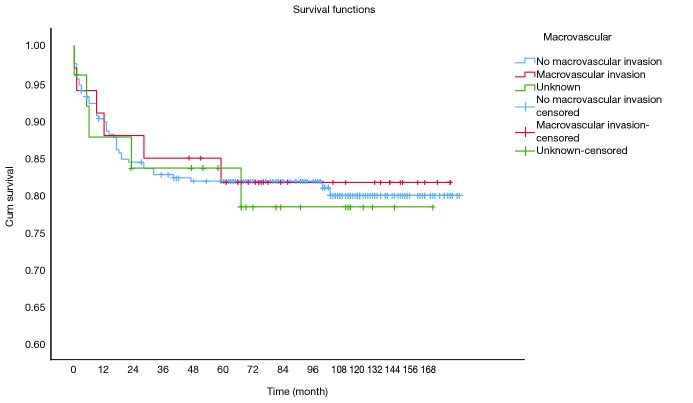
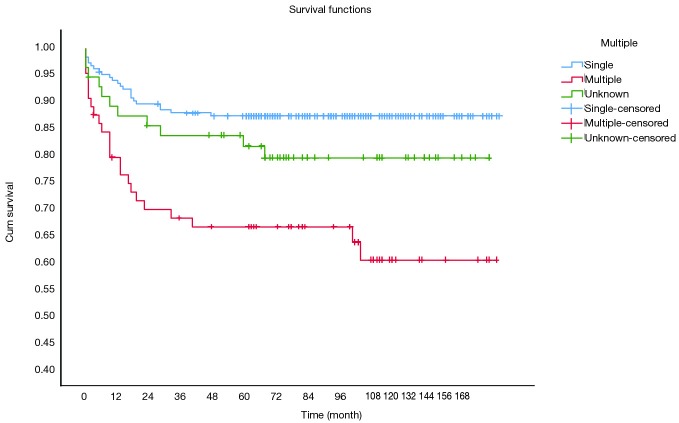
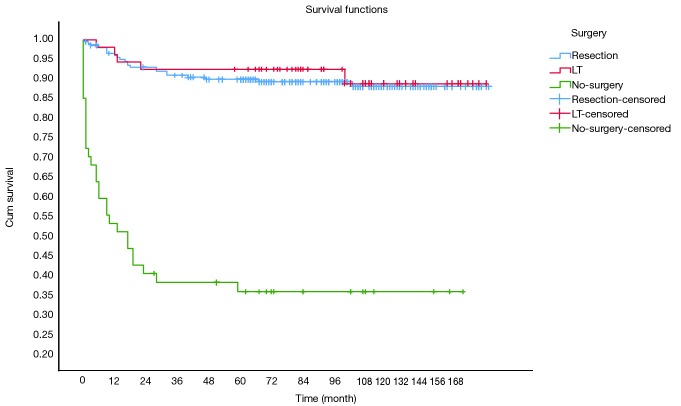
Methods: We calculate age-adjusted incidence of HB by using SEER 21 registries. Age, sex, race, tumor size, macrovascular involvement, multifocal tumor, distant metastasis, the way of treatment, and the survival were collected for survival and analysis of prognostic factors in SEER 18 registries. Survival curves, according to different factors, were obtained by Kaplan-Meier estimates. Multivariable Cox regression models were also built.
Results: The overall age-adjusted incidence of HB was 0.19 patients per 100,000 children with a statistically significant increase per year. Overall survival (OS) at 1-, 3- and 5-year for all patients were 89.3%, 84.6%, and 81.9%, respectively. Multivariate analysis showed tumor size >5 cm [hazard ratio (HR), 8.271; 95% confidence interval (CI), 1.134-60.310], multiple tumors (HR, 2.578; 95% CI, 1.424-4.668) and no-surgery treatment (HR, 7.520; 95% CI, 4.121-13.724) were independent indicators of poor prognosis. Only the age ≥2-year-old (HR, 3.240; 95% CI, 1.433-7.326) and multiple tumors (HR, 2.395; 95% CI, 1.057-5.430) were the risk factors for the surgical treatment group.
Conclusions: The survival of patients with HB has been greatly improved in the recent years, and at the same time, due to the application of better chemotherapy, we should re-evaluate the traditional risk indicators of prognosis in order to better apply to the clinical.
Keywords: Hepatoblastoma (HB); Surveillance, Epidemiology and End Results (SEER); survival.
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources