

Risk Stratification for Postoperative Acute Kidney Injury in Major Noncardiac Surgery Using Preoperative and Intraoperative Data
- PMID: 31808922
- PMCID: PMC6902769
- DOI: 10.1001/jamanetworkopen.2019.16921
Risk Stratification for Postoperative Acute Kidney Injury in Major Noncardiac Surgery Using Preoperative and Intraoperative Data
Abstract
Importance: Acute kidney injury (AKI) is one of the most common complications after noncardiac surgery. Yet current postoperative AKI risk stratification models have substantial limitations, such as limited use of perioperative data.
Objective: To examine whether adding preoperative and intraoperative data is associated with improved prediction of noncardiac postoperative AKI.
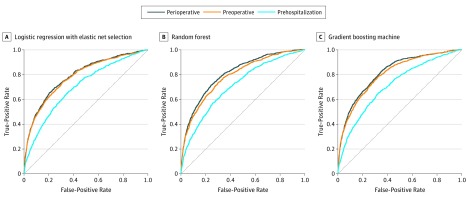
Design, setting, and participants: A prognostic study using logistic regression with elastic net selection, gradient boosting machine (GBM), and random forest approaches was conducted at 4 tertiary academic hospitals in the United States. A total of 42 615 hospitalized adults with serum creatinine measurements who underwent major noncardiac surgery between January 1, 2014, and April 30, 2018, were included in the study. Serum creatinine measurements from 365 days before and 7 days after surgery were used in this study.
Main outcomes and measures: Postoperative AKI (defined by the Kidney Disease Improving Global Outcomes within 7 days after surgery) was the primary outcome. The area under the receiver operating characteristic curve (AUC) was used to assess discrimination.
Results: Among 42 615 patients who underwent noncardiac surgery, the mean (SD) age was 57.9 (15.7) years, 23 943 (56.2%) were women, 27 857 (65.4%) were white, and the most frequent surgery types were orthopedic (15 718 [36.9%]), general (8808 [20.7%]), and neurologic (6564 [15.4%]). The rate of postoperative AKI was 10.1% (n = 4318). The progressive addition of clinical data improved model performance across all modeling approaches, with GBM providing the highest discrimination by AUC. In GBM models, the AUC increased from 0.712 (95% CI, 0.694-0.731) using prehospitalization variables to 0.804 (95% CI, 0.788-0.819) using preoperative variables (inclusive of prehospitalization variables) (P < .001 for AUC comparison). The AUC further increased to 0.817 (95% CI, 0.802-0.832) when adding intraoperative variables (P < .001 for comparison vs model using preoperative variables). However, the statistically significant improvements in discrimination did not appear to be clinically significant. In particular, the AKI rate among patients classified as high risk improved from 29.1% to 30.0%, a net of 15 patients were appropriately reclassified as high risk, and an additional 15 patients were appropriately reclassified as low risk.
Conclusions and relevance: The findings of the study suggest that electronic health record data may be used to accurately stratify patients at risk of perioperative AKI, but the modest improvements from adding intraoperative data should be weighed against challenges in using intraoperative data.
Conflict of interest statement
Figures
References
-
- National Hospital Discharge Survey: 2010 table, Procedures by selected patient characteristics. https://www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedurea.... Published 2010. Accessed October 1, 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
