

Assessment of a Staging System for Sigmoid Colon Cancer Based on Tumor Deposits and Extramural Venous Invasion on Computed Tomography
- PMID: 31808924
- PMCID: PMC6902773
- DOI: 10.1001/jamanetworkopen.2019.16987
Assessment of a Staging System for Sigmoid Colon Cancer Based on Tumor Deposits and Extramural Venous Invasion on Computed Tomography
Abstract
Importance: Preoperative TNM stratification of colon cancer on computed tomography (CT) does not identify patients who are at high risk of recurrence that could be selected for preoperative treatment.
Objective: To evaluate the utility of CT findings for prognosis of sigmoid colon cancer.
Design, setting, and participants: This prognostic study used retrospective data from patients who underwent bowel resection for sigmoid colon cancer between January 1, 2006, and January 1, 2015, at a tertiary care center receiving international and national referrals for colorectal cancer. Statistical analysis was performed in April 2019.
Main outcomes and measures: Cox proportional hazards regression analysis was performed to investigate CT findings associated with disease recurrence. Kaplan-Meier survival plots were calculated for disease-free survival using CT staging systems.
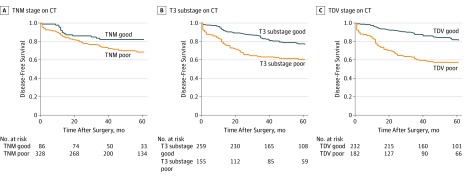
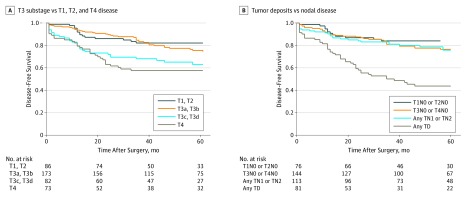
Results: Of the 414 patients who had sigmoid colon cancer (248 [60.0%] men; mean [SD] age, 66.1 [12.7] years), with median follow-up of 61 months (interquartile range, 40-87 months), 122 patients (29.5%) developed disease recurrence. On multivariate analysis, nodal disease was not associated with disease recurrence; only tumor deposits (hazard ratio [HR], 1.90; 95% CI, 1.21-2.98; P = .006) and extramural venous invasion (HR, 1.97; 95% CI, 1.26-3.06; P = .003) on CT were associated with disease recurrence. Significant differences in disease-free survival were found using CT-T3 substage classification (HR, 1.88; 95% CI, 1.32-2.68) but not CT-TNM (HR, 1.55; 95% CI, 0.94-2.55). The presence of tumor deposits or extramural venous invasion on CT (HR, 2.45; 95% CI, 1.68-3.56) had the strongest association with poor outcome.
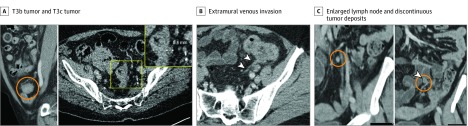
Conclusions and relevance: In this study, T3 substaging and detection of tumor deposits or extramural venous invasion on preoperative CT scans of sigmoid colon cancer were prognostic factors for disease-free survival, whereas TNM and nodal staging on CT had no prognostic value. T3 substaging and detection of tumor deposits or extramural venous invasion of sigmoid colon cancer was superior to TNM on CT and could be used to preoperatively identify patients at high risk of recurrence.
Conflict of interest statement
Figures
Similar articles
-
Performance of CT in the locoregional staging of colon cancer: detailed radiology-pathology correlation with special emphasis on tumor deposits, extramural venous invasion and T staging.Abdom Radiol (NY). 2024 Jun;49(6):1792-1804. doi: 10.1007/s00261-024-04203-0. Epub 2024 Mar 6. Abdom Radiol (NY). 2024. PMID: 38446179
-
Local recurrence in sigmoid cancer is a hidden problem, could CT prognostic factors be of value in their prevention? A multi-centre study of 414 patients.Eur J Surg Oncol. 2021 Aug;47(8):2093-2099. doi: 10.1016/j.ejso.2021.03.254. Epub 2021 Mar 30. Eur J Surg Oncol. 2021. PMID: 33849740
-
Prognostic impact of extramural venous invasion detected by contrast-enhanced CT colonography in colon cancer.BJS Open. 2024 Jan 3;8(1):zrad121. doi: 10.1093/bjsopen/zrad121. BJS Open. 2024. PMID: 38242576 Free PMC article.
-
Evaluation of colon cancer prognostic factors by CT and MRI: an up-to-date review.Abdom Radiol (NY). 2024 Nov;49(11):4003-4015. doi: 10.1007/s00261-024-04373-x. Epub 2024 Jun 4. Abdom Radiol (NY). 2024. PMID: 38831072 Review.
-
The degree of extramural spread of T3 rectal cancer: an appeal to the American Joint Committee on Cancer.Colorectal Dis. 2017 Jan;19(1):8-15. doi: 10.1111/codi.13565. Colorectal Dis. 2017. Retraction in: Colorectal Dis. 2017 Mar;19(3):310. doi: 10.1111/codi.13456. PMID: 27883254 Retracted. Review.
Cited by
-
Correlation and prognostic value of CT-detected extramural venous invasion and pathological lymph-vascular invasion in colon cancer.Abdom Radiol (NY). 2022 Apr;47(4):1232-1243. doi: 10.1007/s00261-022-03414-7. Epub 2022 Feb 8. Abdom Radiol (NY). 2022. PMID: 35133470
-
Performance of CT in the locoregional staging of colon cancer: detailed radiology-pathology correlation with special emphasis on tumor deposits, extramural venous invasion and T staging.Abdom Radiol (NY). 2024 Jun;49(6):1792-1804. doi: 10.1007/s00261-024-04203-0. Epub 2024 Mar 6. Abdom Radiol (NY). 2024. PMID: 38446179
-
Effect of sigmoidectomy in treating sigmoid colon cancer: A protocol of systematic review.Medicine (Baltimore). 2021 Jan 22;100(3):e23914. doi: 10.1097/MD.0000000000023914. Medicine (Baltimore). 2021. PMID: 33545961 Free PMC article.
-
Machine Learning-Based Radiomics Nomogram for Detecting Extramural Venous Invasion in Rectal Cancer.Front Oncol. 2021 Mar 26;11:610338. doi: 10.3389/fonc.2021.610338. eCollection 2021. Front Oncol. 2021. PMID: 33842316 Free PMC article.
-
Tumour deposit count is an independent prognostic factor in colorectal cancer-a population-based cohort study.Br J Surg. 2024 Dec 24;112(1):znae309. doi: 10.1093/bjs/znae309. Br J Surg. 2024. PMID: 39787029 Free PMC article.
References
-
- Burton S, Brown G, Daniels IR, Norman AR, Mason B, Cunningham D; Royal Marsden Hospital, Colorectal Cancer Network . MRI directed multidisciplinary team preoperative treatment strategy: the way to eliminate positive circumferential margins? Br J Cancer. 2006;94(3):-. doi:10.1038/sj.bjc.6602947 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
