

Pharmacokinetics and Pharmacodynamics of Intramuscular and Oral Betamethasone and Dexamethasone in Reproductive Age Women in India
- PMID: 31808984
- PMCID: PMC7070803
- DOI: 10.1111/cts.12724
Pharmacokinetics and Pharmacodynamics of Intramuscular and Oral Betamethasone and Dexamethasone in Reproductive Age Women in India
Abstract
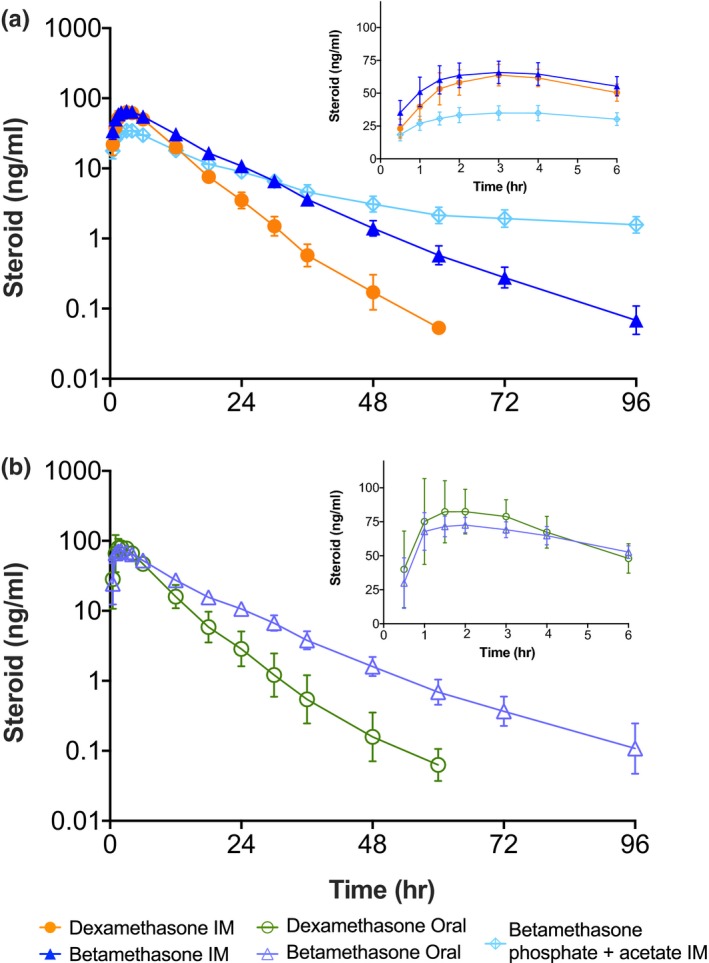
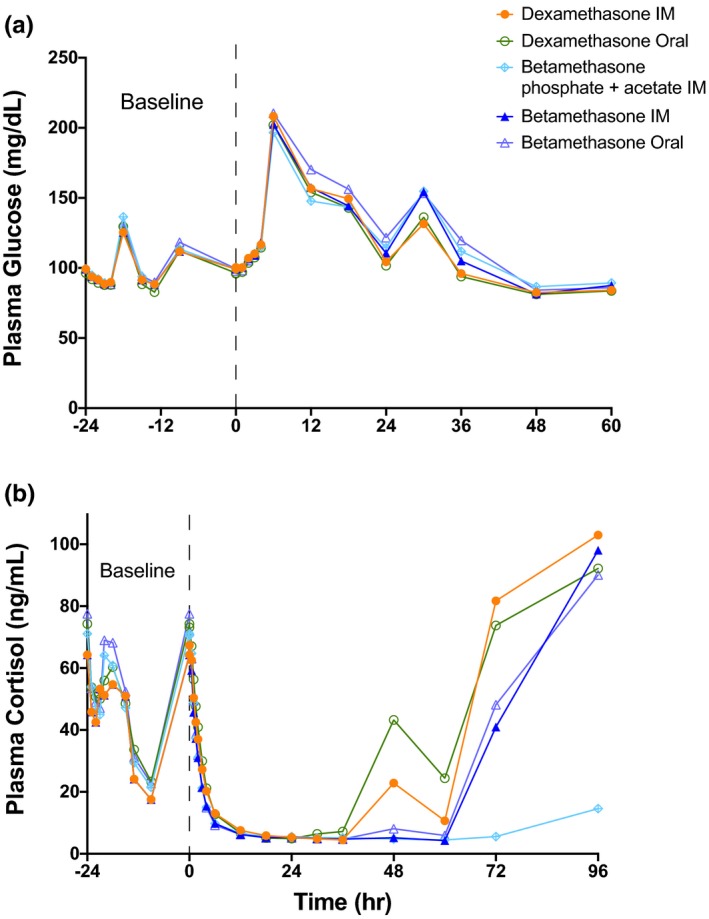
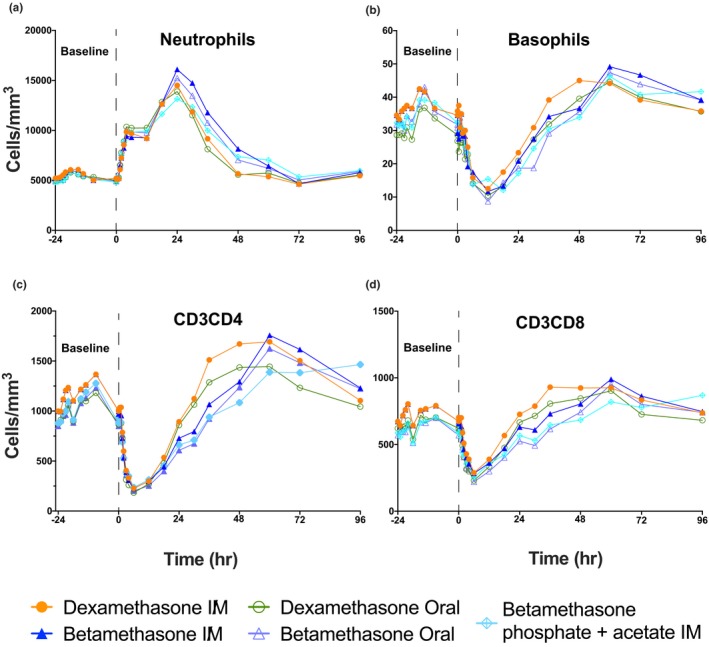
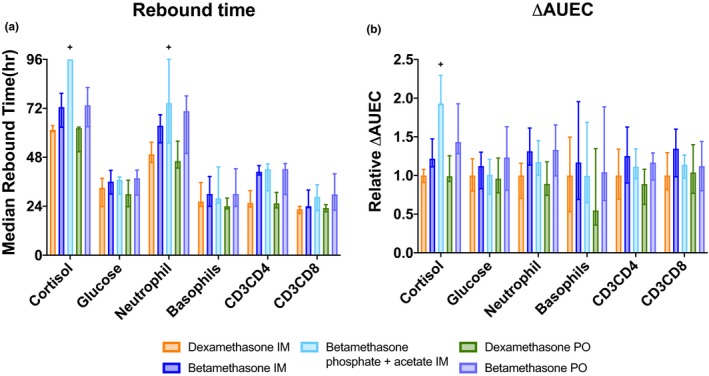
High-dose betamethasone and dexamethasone are standard of care treatments for women at risk of preterm delivery to improve neonatal respiratory and mortality outcomes. The dose in current use has never been evaluated to minimize exposures while assuring efficacy. We report the pharmacokinetics and pharmacodynamics (PDs) of oral and intramuscular treatments with single 6 mg doses of dexamethasone phosphate, betamethasone phosphate, or a 1:1 mixture of betamethasone phosphate and betamethasone acetate in reproductive age South Asian women. Intramuscular or oral betamethasone has a terminal half-life of 11 hours, about twice as long as the 5.5 hours for oral and intramuscular dexamethasone. The 1:1 mixture of betamethasone phosphate and betamethasone acetate shows an immediate release of betamethasone followed by a slow release where plasma betamethasone can be measured out to 14 days after the single dose administration, likely from a depo formed at the injection site by the acetate. PD responses were: increased glucose, suppressed cortisol, increased neutrophils, and suppressed basophils, CD3CD4 and CD3CD8 lymphocytes. PD responses were comparable for betamethasone and dexamethasone, but with longer times to return to baseline for betamethasone. The 1:1 mixture of betamethasone phosphate and betamethasone acetate caused much longer adrenal suppression because of the slow release. These results will guide the development of better treatment strategies to minimize fetal and maternal drug exposures for women at risk of preterm delivery.
© 2019 The Authors. Clinical and Translational Science published by Wiley Periodicals, Inc. on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures
References
-
- Liggins, G.C. & Howie, R.N. A controlled trial of antepartum glucocorticoid treatment for prevention of the respiratory distress syndrome in premature infants. Pediatrics 50, 515–525 (1972). - PubMed
-
- World Health Organization (WHO) . Recommendations on Interventions to Improve Preterm Birth Outcomes (WHO, Geneva, Austria, 2015). - PubMed
-
- Brownfoot, F.C. , Gagliardi, D.I. , Bain, E. , Middleton, P. & Crowther, C.A. Different corticosteroids and regimens for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst. Rev. 8, CD006764 (2013). - PubMed
-
- Jobe, A.H. & Goldenberg, R.L. Antenatal corticosteroids: an assessment of anticipated benefits and potential risks. Am. J. Obstet. Gynecol. 219, 62–74 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
