

Antenatal magnesium sulphate and adverse neonatal outcomes: A systematic review and meta-analysis
- PMID: 31809499
- PMCID: PMC6897495
- DOI: 10.1371/journal.pmed.1002988
Antenatal magnesium sulphate and adverse neonatal outcomes: A systematic review and meta-analysis
Abstract
Background: There is widespread, increasing use of magnesium sulphate in obstetric practice for pre-eclampsia, eclampsia, and preterm fetal neuroprotection; benefit for preventing preterm labour and birth (tocolysis) is unproven. We conducted a systematic review and meta-analysis to assess whether antenatal magnesium sulphate is associated with unintended adverse neonatal outcomes.
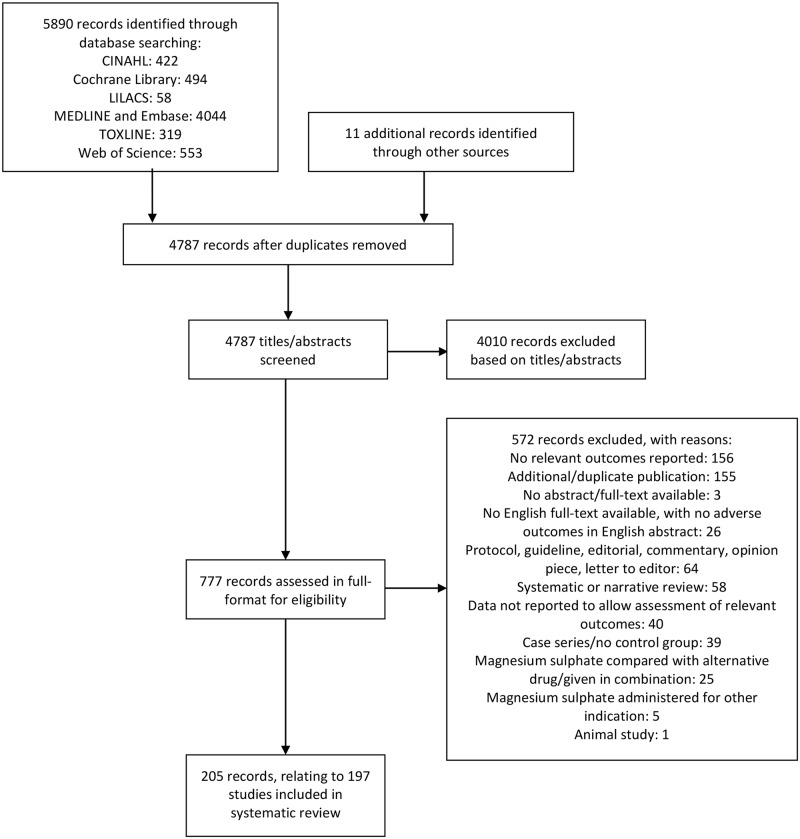
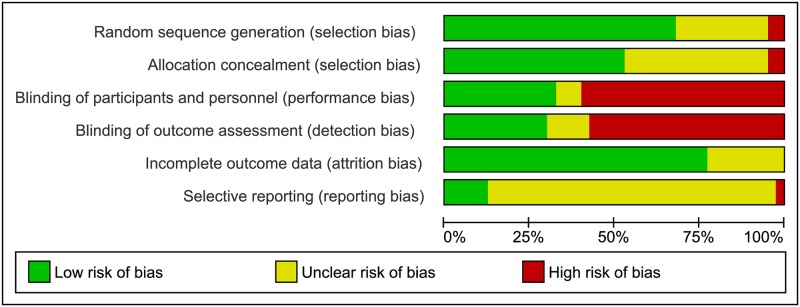
Methods and findings: CINAHL, Cochrane Library, LILACS, MEDLINE, Embase, TOXLINE, and Web of Science, were searched (inceptions to 3 September 2019). Randomised, quasi-randomised, and non-randomised trials, cohort and case-control studies, and case reports assessing antenatal magnesium sulphate for pre-eclampsia, eclampsia, fetal neuroprotection, or tocolysis, compared with placebo/no treatment or a different magnesium sulphate regimen, were included. The primary outcome was perinatal death. Secondary outcomes included pre-specified and non-pre-specified adverse neonatal outcomes. Two reviewers screened 5,890 articles, extracted data, and assessed risk of bias following Cochrane Handbook and RTI Item Bank guidance. For randomised trials, pooled risk ratios (RRs) or mean differences, with 95% confidence intervals (CIs), were calculated using fixed- or random-effects meta-analysis. Non-randomised data were tabulated and narratively summarised. We included 197 studies (40 randomised trials, 138 non-randomised studies, and 19 case reports), of mixed quality. The 40 trials (randomising 19,265 women and their babies) were conducted from 1987 to 2018 across high- (16 trials) and low/middle-income countries (23 trials) (1 mixed). Indications included pre-eclampsia/eclampsia (24 trials), fetal neuroprotection (7 trials), and tocolysis (9 trials); 18 trials compared magnesium sulphate with placebo/no treatment, and 22 compared different regimens. For perinatal death, no clear difference in randomised trials was observed between magnesium sulphate and placebo/no treatment (RR 1.01; 95% CI 0.92 to 1.10; 8 trials, 13,654 babies), nor between regimens. Eleven of 138 non-randomised studies reported on perinatal death. Only 1 cohort (127 babies; moderate to high risk of bias) observed an increased risk of perinatal death with >48 versus ≤48 grams magnesium sulphate exposure for tocolysis. No clear secondary adverse neonatal outcomes were observed in randomised trials, and a very limited number of possible adverse outcomes warranting further consideration were identified in non-randomised studies. Where non-randomised studies observed possible harms, often no or few confounders were controlled for (moderate to high risk of bias), samples were small (200 babies or fewer), and/or results were from subgroup analyses. Limitations include missing data for important outcomes across most studies, heterogeneity of included studies, and inclusion of published data only.
Conclusions: Our findings do not support clear associations between antenatal magnesium sulphate for beneficial indications and adverse neonatal outcomes. Further large, high-quality studies (prospective cohorts or individual participant data meta-analyses) assessing specific outcomes, or the impact of regimen, pregnancy, or birth characteristics on these outcomes, would further inform safety recommendations. PROSPERO: CRD42013004451.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. WHO recommendations for prevention and treatment of pre-eclampsia and eclampsia. Geneva: World Health Organization; 2011. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
